Introduction
Over three decades ago, ultrasound emerged as a promising technique for assessing the thickness and pathologies of cartilage.1 Cartilage pathology is a hallmark of degenerative joint diseases, notably osteoarthritis, which is of paramount concern to physical therapists due to its impact on an athletes pain, mobility and function. The femoral trochlea is an integral component of the knee joint mechanism, and its pathologies are often implicated in anterior knee pain and dysfunction among athletes. The trochlear cartilage serves dual functions as a lubricant and a shock absorber, mitigating the transfer of load to the subchondral bone. Cartilage irregularities frequently underlie anterior knee pain.2 Abnormalities in the trochlea, such as dysplasia, can lead to patellar instability, maltracking, pain, and degenerative changes that impact an athlete’s performance and quality of life. Prompt and accurate assessment of the femoral trochlea is essential for the early detection and management of these conditions. Accurate visualization of the femoral trochlea is essential for diagnosis, treatment planning, and monitoring the healing process in athletes presenting with anterior knee pain or suspected patellofemoral dysfunction.
Historically, the assessment of the femoral trochlea has relied on magnetic resonance imaging (MRI) and computed tomography (CT). These traditional imaging modalities have only offered static views that sometimes fall short in replicating the stresses and movements an athlete’s knee undergoes during dynamic activity. Despite MRI becoming the preferred modality for articular cartilage evaluation due to its superior contrast resolution, there is a resurgence of interest in leveraging MSK ultrasound as an adjunctive tool alongside MRI.3–6 Over two decades ago, it was recognized that ultrasonography could be a viable technique for assessing knee articular cartilage thickness as well as alterations in the surface and subsurface of the cartilage. A substantial corpus of research validates the effectiveness of ultrasound in diagnosing cartilage pathologies. Recent investigations into ultrasonography have yielded reasonably accurate results for the identification of chondral lesions and the measurement of cartilage thickness in animal models.7,8
In contemporary clinical practice, the application of knee MSK ultrasonography is gaining traction as an adjunctive diagnostic tool alongside MRI. In vitro studies have confirmed ultrasonography’s precision in identifying and detailing cartilage defects in both animal and cadaver models, including the accurate grading of induced defects as per the International Cartilage Repair Society’s criteria.7–9 As the condition progresses, the cartilage may exhibit asymmetrical thinning, accompanied by changes in the underlying subchondral bone.
Technical Overview
The assessment of the femoral trochlea via MSK ultrasound involves a systematic approach to imaging. The patient is typically positioned supine with the knee extended or slightly flexed. A high-frequency linear transducer is preferred to visualize the superficial structures of the knee in high definition. The advancements in high-frequency linear transducers have significantly improved the resolution of MSK ultrasound, allowing for exceptional visualization of superficial structures like the femoral trochlea. Sonographically, normal cartilage presents as hypoechoic with a generally uniform thickness.7–12 Initial chondral lesion stages are marked by changes in the ultrasound echotexture, progressing to irregular thinning and evident chondral lesions, with advanced cases involving the subcortical bone.13 In visualizing the femoral trochlea, the patient is typically positioned supine with the knee in various degres of flexion. The physical therapist places a linear ultrasound probe on the anterior aspect of the knee, adjusting the orientation to optimize the view of the trochlear groove. Care should be taken to ensure probe is perpendicular to desired cartilage to decrease risk of anisotropy.
MSK Ultrasound: Technique and Application
Performing an ultrasound examination of the femoral trochlea requires a systematic approach:
-
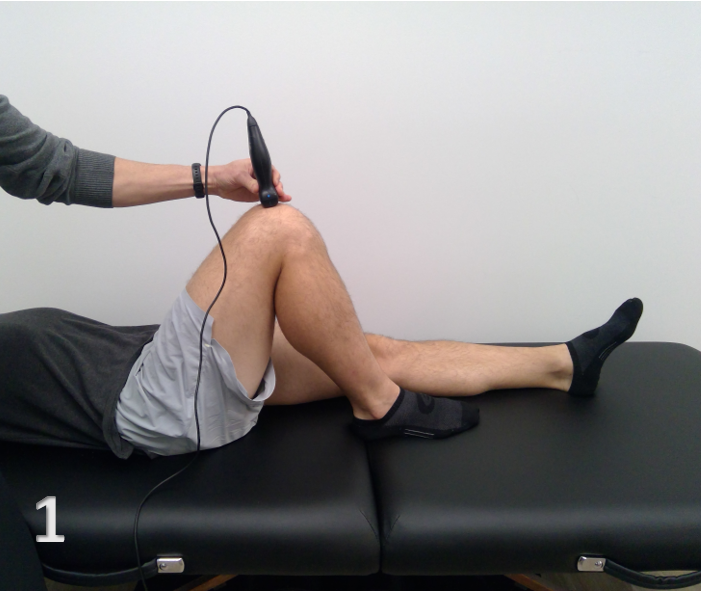
Patient Positioning: The patient is positioned supine with the knee in various degrees of flexion.(Figure 1)
-
Transducer Selection: A high-frequency linear transducer is typically used to optimize the resolution of superficial structures like the femoral trochlea.
-
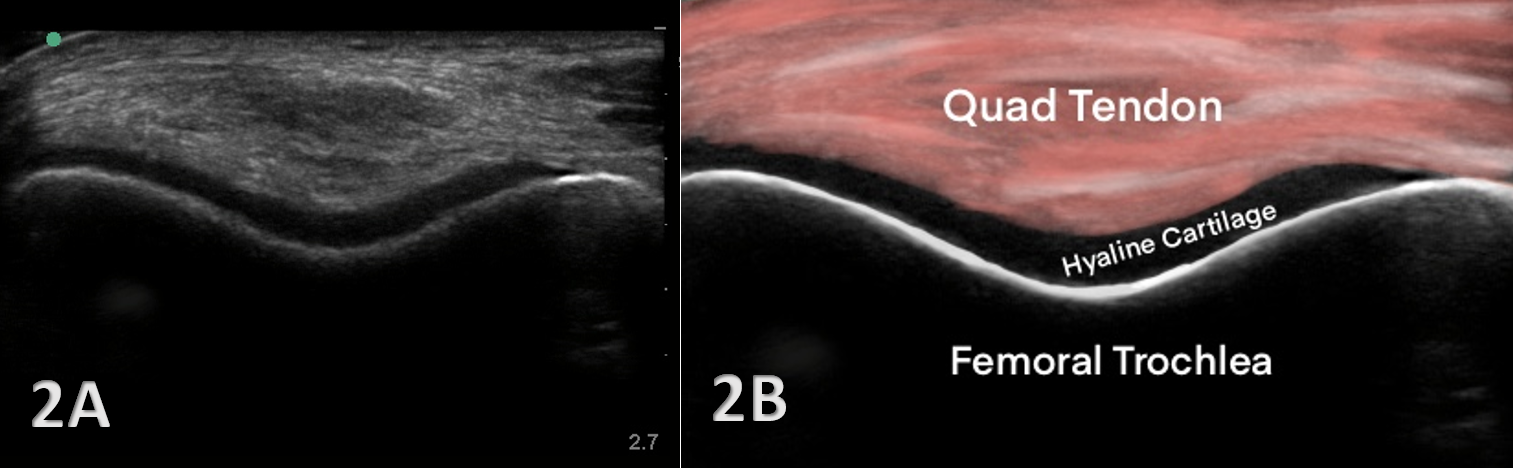
Scanning Technique: The transducer is placed in a transverse/SAX orientation over the distal quadriceps tendon and is then moved distally to the superior pole of the patella, visualizing the trochlear groove. (Figure 2) The capability to conduct sonopalpation (applying pressure with the probe) further assists in assessing the trochlea’s structural integrity and identifying areas of pain or injury.
-
Dynamic Assessment: MSK ultrasound provides immediate feedback on the condition of the trochlear cartilage, subchondral bone, and surrounding soft tissues. It can detect subtle changes in the trochlear surface, synovial tissue, and early signs of patellar maltracking or instability that might be missed during a static examination or with other imaging modalities. Unlike static imaging, MSK ultrasound allows for the observation of the patella’s articulation with the femoral trochlea during dynamic movements. The patient is asked to flex and extend the knee to assess the trochlear tracking and patellar alignment dynamically. This dynamic assessment can be critical for understanding the biomechanical contributions to conditions such as patellofemoral pain syndrome caused by either patellar hyper or hypomobility, and can guide targeted therapeutic interventions.

__short_axis_view.png)
Advantages of MSK Ultrasound in Visualizing the Femoral Trochlea
MSK ultrasound offers several advantages over traditional imaging modalities like MRI and CT scans, including:
-
Dynamic Assessment/Real-time Imaging: MSK ultrasound allows for the observation of the patellar tracking over the trochlea in real-time. The movement of the patella through the trochlear groove can be observed in real-time, providing insights into the functional aspects of the patellofemoral joint that static imaging cannot. High-resolution ultrasound probes can visualize cartilage quality, detecting early signs of breakdown or cartilage wear before they become more significant issues. Therefore, subtle changes in movement can be identified that might contribute to a patient’s symptoms, which static images from MRI cannot capture.
-
Accessibility and Convenience: MSK ultrasound is portable and can be used in various settings, including clinics, sporting events, and on the field. This accessibility allows for immediate assessment and informed decision-making regarding athlete care.
-
Cost-effectiveness: MSK ultrasound is significantly less expensive than MRI and CT, reducing the financial burden on healthcare systems and patients.
-
Safety: The absence of ionizing radiation makes MSK ultrasound a safer choice for repetitive use, particularly in younger populations. It is also non-invasive and generally well-tolerated by patients, with minimal discomfort.
Clinical Implications and Rehabilitation
Visualization of the femoral trochlea through MSK ultrasound has significant clinical implications for sports physical therapy:
-
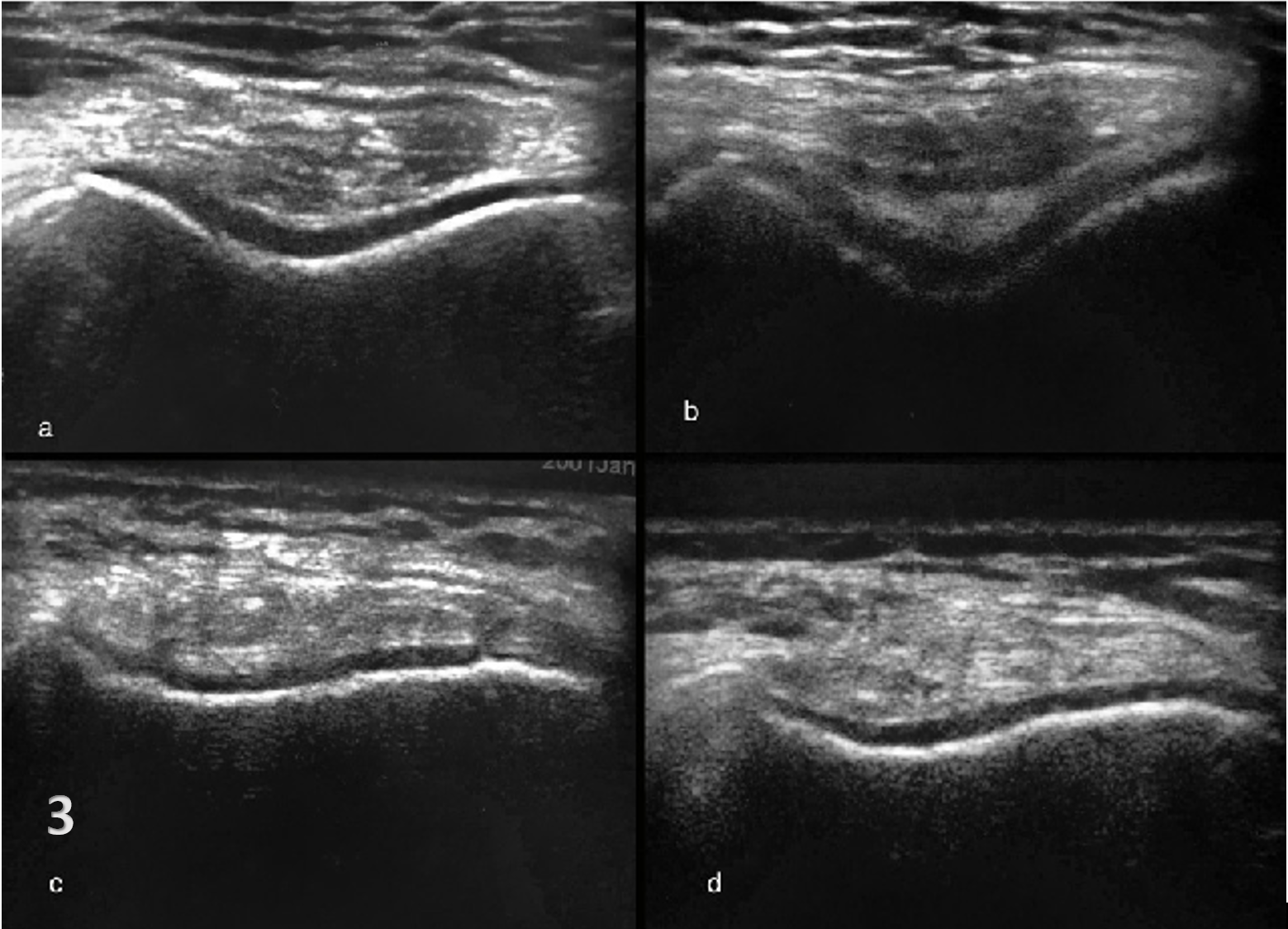
Diagnosis: Early and accurate diagnosis of trochlear dysplasia, cartilage wear, subchondral bone changes, or maltracking can lead to timely and targeted interventions. (Figure 3)
-
Treatment Planning: Real-time imaging helps in guiding interventions such as therapeutic exercises, patellar taping, or ultrasound-guided injections.
-
Rehabilitation Monitoring: Sequential ultrasound examinations can monitor the healing process, assess the efficacy of interventions, and guide the progression of rehabilitation protocols.
-
Injury Prevention: Regular screenings with MSK ultrasound can potentially identify early changes in the trochlear groove, guiding preventive strategies for athletes at risk of patellofemoral disorders.
.png)
Limitations and Considerations
While MSK ultrasound has numerous advantages, there are considerations to keep in mind:
-
Operator Dependency: The quality of the assessment is highly dependent on the skill and experience of the operator. Proper training and practice is essential to ensure accurate and reliable imaging. Proficiency requires significant skill and experience to both acquire and interpret images correctly. A thorough understanding of knee anatomy and proficiency in ultrasound technique are essential for operators.
-
Limited Penetration: Ultrasound may not adequately visualize deeper structures of the knee or those obscured by calcifications. Deep structures and certain pathologies may be better visualized with MRI or CT, necessitating a combined approach for comprehensive evaluation.
-
Patient Factors: Variations in anatomy and the presence of significant soft tissue can affect the quality of ultrasound images.
-
Interpretation Variability: There may be variability in interpretation among clinicians, underscoring the need for standardized training and certification.
Conclusions
Looking ahead, the future of MSK ultrasound, particularly in visualizing the femoral trochlea, appears promising. Advances in technology are expected to overcome some of the current limitations, enhancing the accuracy and ease of interpretation. The increasing interest in femoral trochlear cartilage sonography is attributed to its relevance in the etiology of anterior knee pain and the reality that some patients are either contraindicated for MRI or may prefer ultrasound as a preliminary investigative procedure. MSK ultrasound represents a paradigm shift by offering real-time dynamic imaging, enhancing the evaluation of the trochlear groove and patellar tracking in various states of knee flexion. MSK ultrasound has significantly advanced the assessment and treatment of femoral trochlea pathologies in sports medicine. It enhances the understanding of the patellofemoral joint’s dynamics in real-time, informs clinical decision-making, and augments patient education and engagement. While there are limitations, ongoing advancements in ultrasound technology and clinician education are expected to enhance its application further, solidifying its role in musculoskeletal assessment. As technology advances and proficiency in ultrasound techniques grows, the utilization of MSK ultrasound is poised to become a standard in the assessment of the femoral trochlea, paving the way for more accurate diagnoses and more effective, personalized treatments for athletes.
Future Directions
Ongoing research and technological advancements will likely increase the resolution and capabilities of MSK ultrasound, potentially expanding its applications. One of the exciting developments is the advent of 3D ultrasound. This technology can generate three-dimensional volumetric images, offering a more comprehensive view of the knee joint and its structures, including the femoral trochlea. Furthermore, it can enable a more precise measurement of cartilage thickness and other important parameters, potentially improving the diagnosis and monitoring of disorders like osteoarthritis.
Another promising advancement is the integration of artificial intelligence (AI) and machine learning (ML) into MSK ultrasound. These technologies can assist in image interpretation, reducing the operator-dependency and variability in diagnosis. Moreover, they can potentially automate some of the complex tasks, such as identifying abnormalities or measuring anatomical structures, making the procedure faster and more efficient.
Further research and systematic evaluations are warranted to fully establish ultrasonography’s role in the diagnostic algorithm for knee pathologies. This can help to standardized protocols for trochlea ultrasound assessment, evaluate the efficacy of ultrasound-guided interventions, and help integrate ultrasound findings with other clinical assessments.