INTRODUCTION
Shoulder pain in swimmers has consistently been noted to interfere with swimming training and competition. In 1993, McMaster and Troup published the first large scale United States survey documenting the prevalence of shoulder pain interfering with practice or competition to be 10-26% in a group of 1262 swimmers.1 They also identified aspects of training that swimmers reported aggravated their pain, such as use of paddles, kickboards and stretching. Since that time, additional factors associated with shoulder pain and injury have been studied and the prevalence of shoulder pain in swimmers of varied ages and competitive levels has been well documented.2,3 Given this high pain prevalence, it may not be surprising that a study of baseline shoulder function using the Kerlan-Jobe orthopedic clinic score reported that scores of NCAA swimmers are lower than those of athletes in other overhead sports, and are similar to injured athletes in other sports.4 In addition, except for neurolysis for suprascapular neuropathy, arthroscopic surgery has had limited success in returning swimmers to prior competitive training volume and level.5,6 Therefore, the mainstay of treatment for competitive swimmers is conservative management and Khodaee et al. report that most patients with shoulder pain shoulder cases can be treated with rehabilitation, a proper strengthening routine, and correction of stroke flaws.7
In order to provide appropriate rehabilitation, knowledge of the factors associated with shoulder pain and injury is important for health care providers treating competitive swimmers. Both intrinsic and extrinsic variables have been cited in etiology of shoulder pathology. Extrinsic variables include number of years of swum4,8prior history of shoulder pain or injury,3,9,10 and training variables,8,10 such as acute:chronic workload ratio, which is calculated using the current training volume in relation to the rolling average of the volume of training over the prior four weeks.11–13 A recent systematic review explored the impact of swim volume on various age competition levels and determined that adolescent swimmers experienced the highest level of shoulder pain although adult swimmers had a comparatively higher swim volume.14 Intrinsic factors are specific to the individual swimmer, such as stroke technique, muscle force capacity and endurance, posture and mobility, and, if appropriately identified, may be amenable to change.15 Although stroke characteristics, such as hand entry crossover during freestyle swimming, have been associated with shoulder pain, the videotaping and complex stroke analysis techniques used by researchers may preclude their use in clinical practice.11,12,16 The identification of clinical measures that assess possible contributors to shoulder pain in competitive swimmers is within the scope and ability of most clinicians. While authors have examined which clinical examination findings are related to pain and injury in the swimmers’ shoulder, no systematic review has examined these tools in various age-group and competition levels. Changes in mobility and strength in the musculoskeletal system are inevitable across the lifespan; thus, it is reasonable to expect that risk factors for developing shoulder pain may change over time. Therefore, the purpose of this study was to investigate objective measures utilized to assess swimmers and assess the relationship of test values to shoulder pain in distinct age groups/competition levels. A secondary aim was to identify normative data and/or cutoff values which are associated with risk for swimmers to develop shoulder pain.
METHODS
Study Design
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, and was prospectively registered in Prospero (CRD42021224198)
Search strategy and eligibility
A literature search was conducted by a professional medical librarian (SH) using Medline (via OVID), Embase, CINAHL Complete, SPORTDiscus, and SCOPUS from inception through November 5, 2020. This literature search was updated on May 2, 2022 in order to capture any additional relevant research published since the onset of this project. Search keywords included swimming, shoulder, objective tests and measures. The full search strategy and outcome are summarized in Appendix A. Specific criteria for consideration in the literature search are outlined the Population Intervention Comparison Outcome Time (PICOT) chart in Table 1. Inclusion criteria were articles about swimmers which delineated the age group/competition level, objective tests or measures, and compared measures between groups with and without pain. Exclusion criteria were articles about non-swimming athletes, athletes with history of prior shoulder surgery, studies not reporting on a group that had pain, interventional studies, and non-English publications.
Study selection
Two reviewers (JK and TO) used Covidence systematic review software (Veritas Health Innovation Ltd, Melbourne, Australia) to independently screen titles and abstracts that were identified in the literature search, and the same reviewers screened articles selected for full-text review. Disagreement at the title and abstract review stage as well as the full-text review stage was reached by a third party (AT) who was blinded to the two voters’ selections. Following screening, a hand search of included references was performed to identify articles which may have been missed in the preliminary literature search.
Quality assessment of the included studies
Two reviewers independently determined the study level of evidence using the Oxford Centre for Evidence-Based Medicine levels of evidence from I to V. These two reviewers also independently scored the risk of bias for non-randomized studies using the Methodological Index for Non-randomized Studies (MINORS) tool.17 Consensus on disagreements in score was reached by discussion. The MINORS appraisal tool assigns a score of 0 (not reported), 1 (inadequately reported), or 2 (adequately reported) to eight items for non-comparative studies, and an additional four items for comparative studies. The scores are categorized regarding the quality of study in the following manner: 0-6 is very low; 7-10 is low, 11-16 is moderate, and >16 is strong.18
Data extraction
A custom data extraction sheet was developed using Microsoft Excel (Microsoft Corporation, Redmond, WA), and extraction was performed by three of the investigators (JK, TO and AT). All of the articles underwent a second assessment of data extraction by one of the same three investigators to reach agreement on extracted data.
Extracted data included study characteristics (lead author, year of publication, time to final end point for follow-up, type of study, and sample size) and patient information (gender, age, competition level), all objective tests and measures associated with shoulder pain, and the what the association of objective tests and measures was to the presence of shoulder pain. The swimming competition age level was determined as follows based on a combination of recommended age divisions by the USA swimming competition levels19 and age groupings in included studies was based on the mean reported age to arrive at the following breakdown of age levels of competition:
-
Youth – less than 14 years of age
-
Adolescent/Adult – 15-27 years of age
-
Masters – over 27 years of age
-
Various age levels – the reported ages studied included at least two of the above levels
Data analysis
The agreeability between the two reviewers at the title/abstract and full-text review stages is reported as a Cohen’s Kappa Correlation Coefficient (K).20 A small correlation is said to exist if the K value is <0.4 moderate agreement 0.41-0.6, substantial agreement 0.61-0.8, and nearly perfect agreement 0.81-1.0.
Descriptive analysis was performed for each of the objective tests and measures due to high variance in the methods among studies, and high risk of bias/low quality of evidence for the majority of the studies. The strength of evidence was assigned to each objective test and measure based on publications reporting similar descriptive analysis as summarized in Table 2.21,22
RESULTS
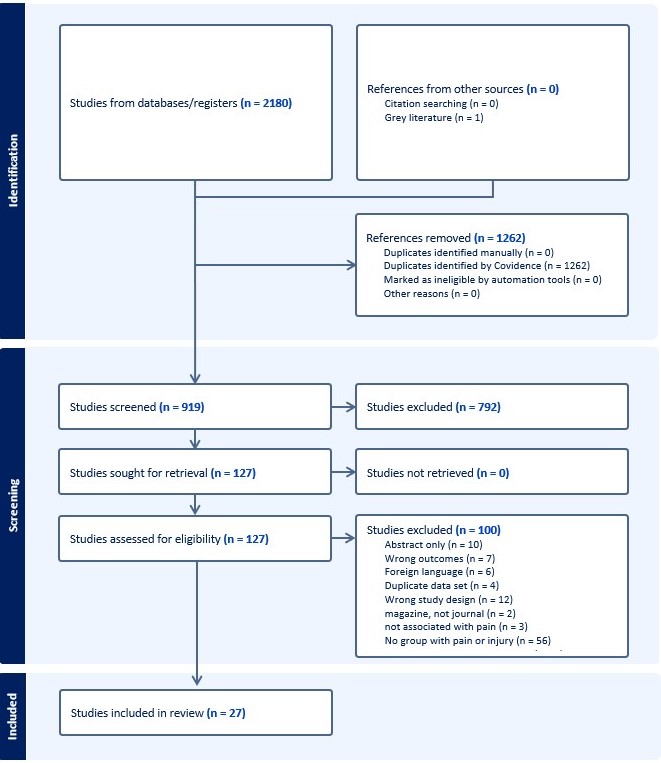
The literature search identified 2180 articles from the data sources, which decreased to 918 studies screened after duplicates were removed. Full text review was conducted on 127 articles. The level of agreement between the two reviewers for the title and abstract phase and full-text review phase was 0.80 and 0.81, respectively, indicating substantial to nearly perfect agreement. Following title and abstract and subsequent full-text review, 22 articles were included for data extraction following the initial search and five additional articles were included after the updated search.3,8,10,12,23–45 Figure 1 provides the PRISMA diagram.

Quality of Evidence
There were four Level IV noncomparative studies that were either case series or prospective cohorts with low numbers,23,27,29,31 12 Level III prospective case-controlled studies,24–26,28,30,32–38 three Level III prospective correlational studies,1,8,45 and seven Level II prospective cohort studies.3,10,11,40,42–44 There were no Level I randomized controlled trials.
The MINORS score for the Level IV studies ranged from 7-10, indicating a low quality of evidence. The MINORS score for the 12 Level III prospective case-controlled studies ranged from 11-19 which indicates an overall strong level of evidence although four of the studies in this category were only moderate level. The three Level III prospective correlational studies had a MINORs score which ranged from 10-15 indicating a moderate level of evidence. The eight Level II prospective cohort studies had a MINORs score which ranged from 9-19 with the majority of the studies demonstrating moderate evidence, and one having strong evidence. The Oxford Levels of Evidence and the MINORs scores for all of the studies included for analysis in this systematic review are provided in Appendix B.
Due to heterogeneity amongst study methods, the overall recommendation for strength of evidence for each objective variable assessed for relationship to shoulder pain is swimmers is reported using the method described above to determine if the overall evidence is strong, moderate limited, conflicting, or no evidence. The summary of objective variables studied, risk of bias, and strength of evidence by age group is detailed in Table 3. The synthesis of the strength of evidence sorted by level of competition is summarized in Table 4.
Internal and External Rotation Strength
Seven studies evaluated the impact of internal and external rotation strength on shoulder pain with four using hand held dynamometry and three using isokinetic testing systems.10,24,27,28,31,32,37 Patient position (eg. Supine or prone, and arm at neutral versus at 90 degrees of abduction) and speed of isokinetic testing were not standardized across the studies. Five of the studies were on adolescent/adult swim levels, and two were on varied age levels. Limited evidence from two low quality studies demonstrated that isokinetic testing of eccentric ER:concentric IR has a positive relationship to shoulder pain in both male and female adolescent swimmers.24,31 The risk of developing shoulder pain was increased 4.5-fold when a preseason value of eccentric:ER:concentric IR was less than 0.68 in one low quality study.31 In conflict with this evidence, three studies which all used hand held dynamometry demonstrated moderate evidence that there was no relationship between the internal:external rotator strength ratios and development of shoulder pain for swimmers in the adolescent/adult age group,28,32,37 and in one study for swimmers of varied age groups including swimmers up to 77 years.10
Scapular position/dyskinesia
The influence of scapular position and/or scapular dyskinesia on shoulder pain in swimmers was assessed in seven studies.10,11,23,35,36,44,46 Methods employed for analyzing the scapula position and dyskinesia included digital inclinometry of scapular position at various points of shoulder range of motion, the Kibler Test for distance from the spinous processes of the seventh and third thoracic vertebrae to the scapula, and visual inspection (dyskinesis present, yes or no). The age groups of the swimmers One study examined youth, four examined adolescents/adults, and two examined varied age ranges. There is limited evidence from only a single study of youth swimmers demonstrating greater shoulder pain with swimming if they did not have a neutral position of the scapula with the Kibler Test.35 In conflict with this finding is limited evidence from one study using Kibler Test44 and one using visual inspection41 which both describe no relationship between scapular position/dyskinesia and shoulder pain for youth swimmers. Moderate evidence for no relationship between scapular position and shoulder pain was determined from two studies across age groups,10,36 one including youth and adolescent/adult swimmers employed digital inclinometry for assessing the scapula at various intervals of elevation36 and the other10 used visual inspection for swimmers across all age levels (age 8-77).
Periscapular muscle strength
Seven studies evaluated the influence of periscapular muscle strength on shoulder pain in swimmers.10,12,32,33,38,42,43 Two studies were on youth swimmers, three were on adolescent/adult swimmers, one studied swimmers across the lifespan (8-77 years), one assessed masters swimmers, and one study assessed both youth and adolescent/adult ages. Handheld dynamometry was utilized to determine the strength of periscapular muscles in three studies, while the posterior shoulder endurance test was used in three studies, and one study did not clearly describe strength testing methods. Overall, there was moderate evidence for no relationship between scapular strength on shoulder pain in swimmers. There is limited evidence from two studies in youth swimmers to support the assertion that decreased scapular strength is associated with the development of shoulder pain.10,12 One study found a decrease in lower and middle trapezius strength,10 and one demonstrated poorer performance on the posterior shoulder endurance test for youth swimmers who developed shoulder pain.12
Core stability/endurance
Five studies utilized various methods for analyzing core stability and endurance as a risk factor for developing shoulder pain.11,26,32,33,41,42 Methods included use of the closed kinetic chain upper extremity test (number of taps), the timed side bridge, timed prone plank, timed ball bridge, and isokinetic peak torque testing for trunk flexion/extension. One study reported on youth swimmers, three were on adolescent/adult swimmers, and one included various age groups There is moderate evidence from two studies in youth swimmers that decreased trunk endurance is associated with the development of shoulder pain.26,42 One of these studies suggested that a time of less than 8.5 seconds for side plank in youth swimmers was a risk factor for developing shoulder pain.42 In contrast, three studies on adolescent/adult swimmers demonstrated moderate evidence that there was no relationship between core endurance and the development of shoulder pain.32,33,41
Thoracic mobility
Two studies assessed the impact of trunk mobility including thoracic rotation44 and trunk flexion/extension41 on the development of shoulder pain in adolescent/adult swimmers. These studies demonstrated limited evidence regarding the impact of trunk mobility as a risk factor for developing shoulder pain.
Internal and External Rotation Range of Motion
The most widely studied objective variable as a risk factor for shoulder pain was shoulder internal and external range of motion which was reported in 11 studies.3,10,24,25,30,32,34,40–43 One of the studies reports on youth swimmers, six report on adolescent/adult swimmers, one on masters, and three on swimmers of various ages. All of the studies except one used goniometry, and measured rotation at 90 degrees of abduction, while one study reported the presence or absence of glenohumeral internal rotation deficiency as “yes or no.” In the adolescent/adult competition level, six studies demonstrated moderate evidence that there was not a relationship between shoulder rotation measures and the development of shoulder pain.24,30,32,34,41,42 In contrast, Walker et al. suggest that excessive ER (>100 deg) or diminished ER (<93 deg) were risk factors for developing shoulder pain in 11-27 year old swimmers.3 In comparison, there is moderate evidence demonstrating that youth swimmers have association between decreased range of motion and shoulder pain, including Tate et al. who examined 8-11 year olds and Mise et al. who examined 14 year-old boys and described that decrease IR and decreased ER, respectively were associated with greater risk for shoulder pain.10,40
Other Range of Motion
Moderate level evidence for having excessive mobility associated with shoulder pain was described in two studies of youth swimmers using novel range of motion methods: one used a total ROM index and found that pain was associated with higher summation of mobility45; the other used a shoulder rotation width index which was associated with shoulder pain if it was decreased in males, and increased in females.40 This index is purported to be an index of comprehensive shoulder motion combining glenohumeral and scapulothoracic movements; it is a measure of the minimal distance between the two hands that are holding a dowel while raising the arms as high overhead as possible without elbow flexion. One study on masters swimmers43 and one on adolescent/adult swimmers30 associated decreased horizontal adduction with shoulder pain. Cejudo et al. propose that a cut point of having less than 39 degrees of horizontal adduction is associated with 3.6 times the risk of developing shoulder pain with swimming in the adolescent/adult age competition level.
Muscle Length
The influence of flexibility of the pectoralis minor muscles on shoulder pain in adolescent/adult swimmers is reported in three studies32–34 and across various age groups in one study.10 There was moderate evidence to support that tightness of the pectoralis minor muscle is associated with shoulder pain in the adolescent/adult swimmer. Both studies reporting on pectoralis minor muscle length measured in centimeters the distance from the tip of the coracoid process to the base of the 4th rib.
Laxity
Laxity was assessed for the glenohumeral joint in six studies by using the sulcus sign or the anterior/posterior drawer sign using a “yes or no” laxity score or using a KT1000 instrument.1,3,8,23–25 Three studies reported on adolescent/adult swimmers and three report swimmers of various ages. There is strong evidence to support that laxity is associated with pain in adolescent/adult swimmers and in swimmers of various ages.1,8,24 In contrast, two studies provided conflicting evidence demonstrating no association between laxity and shoulder pain for swimmers of various ages.3,25
DISCUSSION
The primary aim of this systematic review was to investigate objective measures utilized to assess swimmers and assess the relationship of these assessments to shoulder pain in distinct age groups/competition levels. The majority of the studies were prospective cohorts of moderate quality with several being high quality and several low quality. A qualitative synthesis of data was conducted due to heterogeneity of methods of obtaining the objective measures. The secondary aim of determining specific cut off values for risk factors in objective measures was achieved in that several values are reported; however, these have not been tested for validation in other studies.
Youth Swimmers
Youth swimmers had shoulder pain associated with scapular dyskinesis (limited evidence for positive relationship), decreased periscapular muscle strength (limited evidence for positive relationship), reduced core endurance (moderate evidence for positive relationship), internal and external rotation ROM (moderate evidence of relationship if decreased IR or increased ER); and laxity (moderate evidence for positive relationship). A cutoff of <8.5 seconds for side plank was proposed for associated of shoulder pain developing in one study, but this has not been tested for validity in other studies. The trend in these findings suggests that youth swimmers may benefit from more strengthening and neuromuscular control exercises to optimize shoulder stability which may be more lax in this skeletally developing age group.
Adolescent swimmers
The majority of studies reported objective measures on adolescent/adult swimmers. This age group had increased risk of shoulder associated with ER:IR strength ratio when eccentric ER and concentric IR were assessed using isokinetic equipment, with a proposed cut off ratio of <0.68 associated with risk of developing shoulder.31 This cut-off ratio is also only reported in one study and has not been tested for validity. Moderate evidence for the adolescent/adult swimmers’ ER and IR strength in one static position using handheld dynamometry demonstrated no relationship with shoulder pain development. The conflicting evidence between these strength tests in this age group is likely attributable to the differing methods of assessing strength. Isokinetic strength testing may be a more accurate reflection of the demands of strength needs for swimmers and a better objective test than handheld dynamometry since the testing demonstrates strength throughout the range of motion and can assess both eccentric and concentric muscle strength. It is possible that eccentric posterior cuff activity compared to the concentric internal rotator contractions reflects the swimmer muscle activation patterns more closely than static measures of strength in one position with handheld dynamometry. The role of the scapula in the development of shoulder pain remains unclear in this age group as noted with conflicting evidence. Tightness of the pectoralis minor was associated with shoulder pain, and this may be related to the pectoralis minor creating an anterior scapular tilt which can contribute to impingement of subacromial structures.47
Masters swimmers
Masters swimmers were only represented in one study43 and therefore the ability to synthesize evidence was not attempted for this age group.
Swimmers assessed across varied age levels of competition
The discrepancy of the role of laxity for swimmers across varied age levels may be related to the wide spread of ages represented in these studies. It is possible that younger swimmers may struggle more with laxity as noted in the youth and adolescent age levels,1,8,24 while older swimmers may not have as much trouble due to the glenohumeral joint becoming less lax with aging. A clinical inference from this could be that youth and adolescent swimmers would benefit from performing band stability exercises, while older swimmers might benefit more from stretching.
A recent systematic review assessed the association of symptom development with objective measures in all regions of the body in elite swimmers, however there was no delineation of age or competition level in that review.48 The authors reported on 17 studies for the upper extremity with similar scores on the MINORs risk of bias assessment to findings in this review which reflect overall moderate levels of evidence. Similar conclusions are reported regarding insufficient evidence regarding scapular static and dynamic positioning on the influence of shoulder pain, and those authors relate the lack of conclusive evidence to the diverse methods of assessing scapular position. The ecc ER:con IR ratio was also supported by moderate evidence in the recent systematic review with one study reporting that a ratio of >1.08 is associated with injury risk24; however, this cut point has not been validated in any prospective studies.
Limitations
Limitations of this systematic review include that only studies in English were included which may have resulted in studies having been excluded. Also, the heterogeneity of data collection methods precluded data pooling in meta-analysis. However, the rigorous method of synthesizing evidence based on the quality of studies allows for meaningful conclusions regarding objective tests for the varied age levels of competition.
Conclusion
Objective tests and measures have been identified which are related to the development of shoulder pain in swimmers of distinct age/competition levels. These clinical tests may prove helpful to assist providers in considering interventions which may prevent the development of shoulder pain. Further research is needed to assess the validity of identified test cut points, and to add to the data pool for the masters level swimmer.
Conflicts of Interest
The Authors report no conflicts of interest.