INTRODUCTION
A concussion is defined as a traumatic brain injury induced by biomechanical forces.1 It is estimated that 1.6-3.8 million sports-related concussions (SRCs) are sustained each year – with up to 60% of these cases presenting with vestibular and oculomotor dysfunctions.2 Common complaints related to vestibular abnormalities include dizziness, impaired balance, vertigo, difficulty in busy environments, and motion discomfort.3 Vision, somatosensory, and vestibular systems are responsible for postural stability and dynamic balance. Thus, deficits in one or more of these systems would result in difficulty maintaining one’s balance. A component of the vestibular system, the vestibulospinal reflex (VSR) coordinates movements of the head and neck with the body in order to maintain the head in an upright position – for example as the head tilts to the left or right.4
The Head Shake-Sensory Organization Test (HS-SOT) was developed from the original Sensory Organization Test (SOT) with the purpose of measuring an individual’s ability to use vestibular input to maintain balance while moving the head.5 The HS-SOT has been examined under different parameters in several populations including: young healthy adults, young adults with peripheral vestibular hypofunction, young athletic populations, and an aging population.6–9 The HS-SOT was evaluated in a healthy population in a study performed by Cripps et al. where the test-retest reliability was found to be excellent (0.78-0.85) in healthy asymptomatic adults aged 20 to 26 years.10 Honaker et al. tested individuals with and without peripheral vestibular asymmetry to determine the sensitivity and specificity of the HS-SOT for indicating peripheral vestibular hypofunction.7 It was determined that the sensitivity of Condition 5 of the HS-SOT with horizontal head turns at 15 degrees per second was 70%, and the specificity was 100%.7 This suggests the effectiveness of Condition 5 of the HS-SOT with head turns of 15 degrees per second for confirming peripheral vestibular dysfunction, or asymmetry. Another study confirmed the reliability of the HS-SOT in healthy young adults (ICC=0.85, 0.78 for Conditions 2 and 5 respectively) compared to lesser reliability in older populations.5 The HS-SOT has not been tested in populations with a known history of concussion. Because vestibular dysfunction has been implicated in those with concussions, clinical tools should be used to fully assess the resulting impairments. The purpose of this study was to compare the performance of adults with no history of concussion to those with a history of concussion on the Head Shake-Sensory Organization Test to determine if long-standing balance deficits are present after concussion.
The hypothesis is that individuals with a history of concussion will score lower (not as well) than those without a history of concussion.
METHODS
This cross-sectional study was approved by the Northern Arizona University Institutional Review Board and all subjects gave informed consent.
Participants
Participants were recruited through flyers distributed to a public university in a metropolitan community. Participants were required to be 18 to 35 with a history of concussion(s) or no history of concussion(s) and possess sufficient English language skills to complete questionnaires. Participants were excluded if they were: under 18 or over 35 years, had a lower extremity musculoskeletal injury in the prior three months; history of a head injury in the past year; or diagnosis of a visual, vestibular, or balance disorder, had limited cervical range of motion that would interfere with horizontal head movements, were unable to complete the SOT or had fall reactions to SOT Conditions 5 and 6, had an acute concussion within seven days of participation in the study, had a history of migraines or severe motion intolerance. Participants were had to have not consumed alcohol for 24 hours before participating in testing.
Telephone screening was used to ascertain eligibility. Participants meeting study criteria were provided information about the purpose of the research and the potential risks. Participants provided written informed consent. Experimental procedures were approved by the institutional review board associated with the study. Participants completed a personal/medical history form prior to testing to ensure there were no reasons for exclusion.
Instrumentation
Sensory Organization Test (SOT)
The SOT evaluates sensory interactions during six conditions that selectively remove or disrupt visual, somatosensory, or vestibular systems with the participant attempting to maintain steady state standing balance while wearing a harness. The conditions are the following: (1) eyes open standing on a firm surface; (2) eyes closed while standing on a firm surface; (3) sway-referenced vision standing on a firm surface; (4) eyes open standing on a sway-referenced surface; (5) eyes closed standing on a sway-referenced surface; and (6) eyes open, sway-referenced vision standing on a sway-referenced surface. Three trials are performed for each condition to generate a composite equilibrium score. The SOT uses a computerized system with a servo-controlled dual force plate and visual surround to determine whether an individual can effectively use inputs from visual, somatosensory, and vestibular systems to maintain balance while suppressing inaccurate sensory information .11,12 The SOT was performed using the NeuroCom Equitest BalanceMaster, following a standardized procedure in the literature (NeuroCom International, Inc., Clackamas, OR, USA.13 The SOT has good-to-moderate test-retest reliability and has assessed sensory contributions to balance control in children, young adults, older adults, and individuals with neurological disorders.14–17 It has also been used to evaluate the effectiveness of interventions for improving balance.18–20 Although the SOT is a commonly used balance assessment tool, its ability to detect subtle balance deficits has been challenged.19,21–23
Head Shake Sensory-Organization Test (HS-SOT)
The HS-SOT is an enhancement of the SOT and was developed to improve the delineation of balance performance.5,24,25 In the HS-SOT, dynamic head movements are incorporated into standard SOT Condition 2 and Condition 5.5,24 Unlike the SOT where the head is static, the HS-SOT requires active head movements in the horizontal plane, as if saying no repeatedly, to correspond with visual and auditory feedback while maintaining a fixed head velocity at approximately 100° per second as measured by an accelerometer. In addition to assessing the possible influence of head movements on postural stability, the HS-SOT also stimulates the semicircular canals.24 This stimulation creates additional vestibular input that must be integrated during the balance task.25 Therefore, the HS-SOT may expose subtle balance deficits and enhance the clinical standard use of the SOT.5 The HS-SOT has been shown to have excellent test-retest reliability in healthy, younger adults and moderate-to-good test-retest reliability in healthy, older adults.26 At least five separate trials of each condition of the HS-SOT are required to calculate composite fixed (Condition 2) and sway (Condition 5) scores.
The Dizziness Handicap Inventory (DHI)
The DHI is a self-assessment questionnaire intended to measure the impact of dizziness on an individual’s everyday functioning. The DHI questionnaire has 25 questions about the physical, emotional, and functional effects of dizziness on a person’s life.27 Three subscales are assigned to the questions. The physical subscale consists of nine items that measure the physical effects of vertigo, such as unsteadiness, loss of balance, and nausea. The emotional subscale consists of nine items that measure the emotional effect of vertigo, such as anxiety, depression, and frustration. The functional subscale is comprised of seven items that measure the impact of vertigo on daily activities, such as walking, driving, and working. The overall score runs from 0 to 100, and each question is graded on a 3-point scale (yes, sometimes, no). Higher ratings reflect a larger impact of vertigo on the individual’s everyday life. The DHI can be used to measure the severity of vertigo and to monitor symptomatic changes over time.27
The Activities-Specific Balance Confidence (ABC) Scale
The ABC scale is a questionnaire developed to measure a person’s confidence in their ability to conduct a variety of daily activities without losing their balance or falling. The 16-item ABC scale asks individuals to assess their confidence in accomplishing particular tasks on a scale ranging from 0% (no confidence) to 100% (complete confidence).28 The items encompass a variety of tasks, such as walking up and down stairs and reaching for an object on high shelves. Higher scores on the ABC scale indicate greater trust in balancing.28
Procedures
All testing was conducted at a university research laboratory at the same location and completed in a single session. Participants were permitted to use glasses or contact lenses. Participants completed a personal/medical history form, the DHI, and the ABC. Instructions were provided before each test was performed, and participants were asked to demonstrate their understanding of the test before proceeding. Participants were offered rest breaks and water between tests to ensure hydration and adequate rest. Per SOT manufacturer recommendations, participants were placed in an appropriately sized harness that did not restrict sway, and their malleoli were aligned with the axis of rotation based on their height. Participants were told to stand as steadily as possible while performing SOT Condition 2 (standing eyes closed on fixed surface) and SOT Condition 5 (standing eyes closed on sway surface) under three conditions. The three conditions were the standard SOT protocol, the HS-SOT protocol, and the HS-SOT protocol while standing on a foam pad. The order of the three conditions was randomized for each participant. Three trials of the SOT were performed for each condition to calculate a composite score, ranging from 0 to 100. A score of 0 was given to participants who required the harness to prevent a fall.
After completing each of the three conditions, participants were disengaged from the BalanceMaster and offered a seated rest break. Participants were assisted in donning the head accelerometer, and their malleoli were realigned in the proper axis. Participants were instructed to move their head in the horizontal axis at a velocity of approximately 100° per second that corresponded with an auditory tone and visual feedback on the computer monitor. Participants practiced maintaining the horizontal cervical spine motion at the appropriate velocity using the visual feedback until they were able to maintain the motion with their eyes closed and using the auditory feedback. Three trials of each condition were performed to calculate the composite fixed and sway scores.
Statistical analysis
A sample size calculation was performed to estimate modest relationships between the SOT and HS-SOT tests using PASS version 12 software indicating 24 participants would be required for a power of at least 0.80. (NCSS Statistical Software, Kaysville, UT). A p-value of less than .05, two-tailed was considered statistically significant. SPSS version 23.0 (IBM Corp., Armonk, NY) was used to analyze the data. A linear mixed-effects model was performed as the groups were unbalanced. A post hoc analysis was completed to identify any differences between the groups.
RESULTS
Twenty-five individuals participated: nine patients with history of concussion (20.33 +/- 3.35 years, age range: 18–28) and 16 healthy controls (21.50 +/-4.52 years, age range: 18–33). The groups were not significantly different. (Table 1).
The participants’ equilibrium scores during each balance test are presented in Table 2.
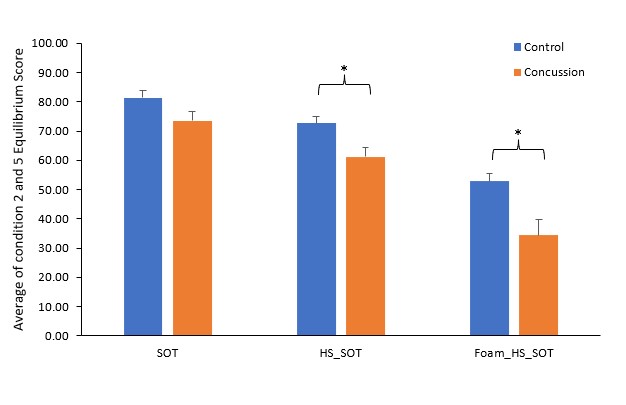
The linear mixed model (3 Tasks x 2 SOT conditions x 2 groups) showed that there was a significant effect of task, F (2, 100.584) = 55.372, p < 0.001, a significant effect of SOT condition, F (1, 98.930) = 179.653, p < 0.001, and a significant effect of group, F (1, 28.367) = 14.701, p < 0.001. No significant 2- or 3- way interactions were found (p > 0.05). A post hoc analysis of task effect with Sidak adjustment showed that the average equilibrium scores (average of SOT2 and SOT5) in both groups significantly decreased with more complex tasks. Furthermore, the concussion group had significantly worse equilibrium scores than the control group during HS-SOT (p = 0.007) and Foam HS-SOT (p = 0.002) tasks but not during the standard SOT task (See Figure 1).

In the patient group, there was a significant within-subject effect between the tasks (F (2, 97.66) = 42.96, p < 0.001), with higher average equilibrium scores observed on standard SOT (81.41, 95% CI: 76.60–86.21) than HS-SOT (72.62, 95% CI: 67.81– 77.42) and both SOT and HS-SOT showed higher average equilibrium scores than Foam-HS-SOT (M = 52.90, 95% CI: 47.48– 58.32).
DISCUSSION
The main findings were that the SOT equilibrium score decreased with the addition of head shake and decreased further when participants stood on the foam cushion, and equilibrium scores of participants with a history of concussion were lower during HS-SOT as well as Foam-HS-SOT than scores of healthy participants. However, no group differences were found during SOT. The results of the current study are clinically important because standardized postural stability tests may not detect subtle differences of disruption of the integration of vision with the vestibular system needed to maintain balance.
Researchers have reported that the HS-SOT has good reliability and may be more useful in discriminating subtle postural instability in healthy younger adults compared to healthy older adults.5,7 Park et al. investigated SOT and HS-SOT performance in adults aged 20 to 39, adults aged 40 to 59, and older adults aged 60 to 79 reporting decreased performance on Condition 5 for the SOT and HS-SOT compared to Condition 2 for the SOT and the HS-SOT.25 The current study differs from these studies by the addition of a foam cushion to increase the difficulty and by focusing on healthy younger adults that had sustained a concussion and comparing differences in healthy younger adults that did not have a concussion.
In the clinic, clinicians often assess balance of a patient by challenging balance such as asking a patient to stand on one leg or by the use of a foam cushion. A foam cushion distorts somatosensation and forces the use of vision and the vestibular systems. The literature is sparse on comparing foam cushions to challenge balance. A foam cushion is used in the concussion balance test (COBALT). DeFeo et al. investigated differences between the SOT, modified Balance Error Scoring System, and COBALT.29 In the DeFeo study, the COBALT involved yaw plane head shaking in healthy younger adults and the authors reported that the COBALT may be a clinically feasible test of sensory integration but this study did not involve patients with a concussion. Massingale et al. compared uninjured (mean age of 14.7) to concussed adolescents (mean age of 15) using the COBALT.30 The foam pad that is used with the COBALT has a foam density of 3.6 lb/cu ft and is 18 inches wide by 20 inches depth by 4 inches in height. The foam pad used with COBALT differs from the NeuroCom foam pad as the NeuroCom foam pad is 18 inches wide by 18 inches depth by 5 inches in height. Chaikeeree et al. have investigated differences in foam pads during static standing and reported the NeuroCom foam pad as having a higher Young’s modulus (0.049 MPa) compared to three different types of foam pad.31 Chaikeeree et al. noted that foam pad selection matters and that the NeuroCom foam pad induced greater sway in both the anterior-posterior direction and medial-lateral direction compared to three other types of foam pads: ethylene vinyl acetate foam, memory foam, and sponge coated with a plastic sheath.31 A comparison of COBALT foam pad to the NeuroCom foam pad has not been studied to the authors knowledge. In the Massingale et al. study, only 55% of the concussed adolescents were able to complete all domains of the COBALT due to an increase in symptoms of dizziness or inadequate neck range of motion.30 If concussed adolescents were unable to complete all of the domains of the COBALT, then it may be too difficult to complete and perhaps the NeuroCom foam pad may be a good substitute. Future studies could compare foam pad cushions.
In the current study, the two patient reported outcome measures used were the DHI and ABC scores. Interestingly, there were no differences in DHI and ABC scores between the control (mean age 21.50 +/-4.52 years) and the concussed (mean age 20.33 +/- 3.35 years) groups. As these subjective outcome measures are measuring perceived dizziness (DHI) and perceived confidence in balance (ABC) across functional activities in 20-year-olds, perhaps the young adults did not perceive to have dizziness or lack confidence in balance during functional activities. Specific to the control group, there were two participants that influenced the overall mean for the control group with one participant noting a DHI score of 4 and a separate participant noting a DHI score of 10. Although the participants did not have a history of concussion it is apparent that these two participants may have misinterpreted the questions relative to a complaint of dizziness. An example of this is question 2 of the DHI that asks “because of your problem, do you feel frustrated” or question 7 that asks “because of your problem, do you have difficulty reading?” Perhaps the participant interpreted these questions without considering that this questionnaire was only relevant to dizziness. The exclusion criteria for the study did not limit those with attention deficit disorder or a learning disability so it is possible that this influenced these two participants, but this information was not collected in this study.
Limitations
There were potential limitations in the current study. First, there was a small sample size of prior concussed participants. When considering the number of concussions reported in an athletic season, the Centers for Disease Control estimates that five to 10% of athletes will be diagnosed with a concussion.32 In the current study, 36% of the participants had a concussion history and were not athletes. The authors of the current study suggest that future studies should investigate a larger athletic population using the HS-SOT to identify potential subtle balance deficits. Second, the National Collegiate Athletic Association and the Department of Defense Concussion Assessment, Research, and Education (NCAA-DOD CARE) trials investigated the impact of attention deficit/hyperactivity disorder, learning disability, and the combination of these two neurodevelopment disorders.33 The NCAA-DOD CARE trial suggests that athletes with these neurodevelopment disorders have a greater risk of incurring a concussion (Relative Risk range of 1.369 to 2.243) compared to controls.33 In the current study, these neurodevelopment disorders were not assessed and therefore it is possible that participants with these disorders were included in the study. It is currently unknown how neurodevelopment disorders impact postural stability in this population. A limitation of the current study is that it was performed in a controlled research lab as the SOT and the HS-SOT conditions are impacted by noisy environments such as the athletic training room. Authors have suggested that both the SOT and HS-SOT should be performed in a quiet environment as participants are attempting to maintain their balance and uncontrolled noise may startle the participant and impact their ability to maintain their balance.5–7 Results may differ in more typical athletic environments.
CONCLUSION
Standardized postural stability tests are commonly used to assess balance deficits; however, these tests may not be sensitive enough to detect subtle differences in balance disruption. In the current study, the HS-SOT and Foam-HS-SOT conditions were more challenging than the SOT for the participants suggesting that the addition of head motion or a foam cushion may assist with identification of balance impairments. Participants with a concussion history had lower equilibrium scores in the HS-SOT and Foam-HS-SOT conditions than healthy participants. This suggests that these tests discriminate subtle postural instability in individuals with a concussion. Clinicians should consider using more challenging postural stability tests to better assess balance deficits in individuals with a concussion.
Conflicts of interest
The authors have no conflicts of interest to report. The authors have no sources of funding to declare.