INTRODUCTION
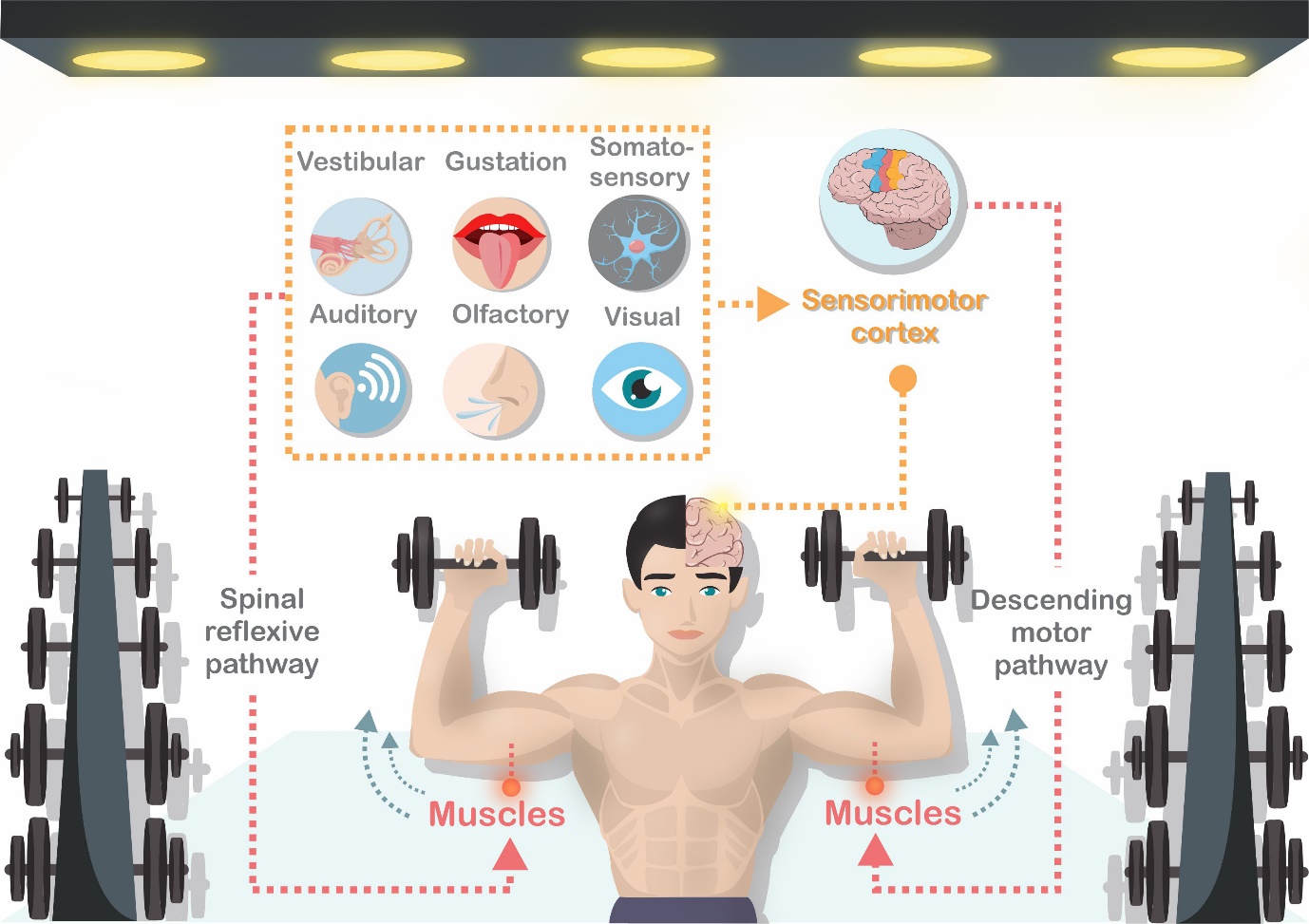
The sensorimotor system is complex and a central element of the body’s motor control system.1–3 It assists with the planning and execution of movement and maintaining postural control (Figure 1).3 It encompasses afferent sensory pathways, efferent motor pathways and central cortex processing (Figure 2). Sensorimotor functioning is required for every movement; requiring integration of sensory information (in particular somatosensory and visual information) to detect deviations from desired orientations and to subsequently alter motor responses.4 Given that movement control requires sensorimotor function, as the complexity of movement increases, for example responding to more stimuli in the environment and/or utilising more multiplanar joint actions or muscles, the sensorimotor demands also increase.5 Therefore, sensorimotor dysfunction, which can occur following musculoskeletal injury (such as anterior cruciate ligament [ACL] injury), may negatively affect movement planning and execution.6,7


The ACL provides: (1) structural stability through limiting excessive tibia anterior translation and internal rotation8,9 and (2) sensory information to the sensorimotor cortex.10,11 Therefore, ACL injury has negative consequences for knee structural stability12,13 and sensorimotor system functions (such as postural control, muscle coordination and supplying afferent information to the central cortex).14–16 Despite ACL reconstructive surgery (ACLR) restoring structural stability,17–21 there is growing debate to whether sensorimotor dysfunction remains. Sensorimotor dysfunction following ACLR occurs across afferent sensory, central processing and efferent motor pathways.22–24 Recent reviews have reported dysfunction of the efferent pathways24–26 and certain aspects of that somatosensory system (proprioception and kinaesthesia).27,28 Whilst there are six sensory systems within the afferent system (somatosensory, visual, auditory, vestibular, gustation and olfactory), the somatosensory and visual systems are the most important for motor control6,29 and will be reviewed here.
The somatosensory system has several important functions, including: (1) informing the central cortex about segment position (proprioception) and movement (kinesthesia), (2) sensing pain and pressure/vibration, and (3) sensing objects in the environment via touch.30 The ACL is highly innervated with mechanoreceptors that send proprioceptive afferent information for processing to the spinal cord, lower brain and cerebrum.10,11 A full-thickness ACL tear results in disruption of the mechanoreceptor mediated pathway,31 pain and swelling, thereby driving arthrogenic muscle inhibition.32,33 While two systematic reviews have investigated proprioception deficits (one domain of the somatosensory system), which highlighted significant but small functional reductions following ACLR,27,28 no study has reviewed the other somatosensory system domains (e.g. central processing and vibration).
The visual system encompasses the eyes, optical neural pathways and the occipital lobe (where processing of the visual information occurs). It has several key functions, including helping to identify objects and providing object spatial location and orientation within their environment.34 Following the loss of ACL proprioceptive information, postural control is reduced with increased demands placed on motor planning centres within the brain. In particular, an over-reliance on the visual system can occur following ACLR and may contribute to ACL reinjury.35 While early research into visual system dysfunction was based on functional brain MRI,35,36 there is a small but growing body of research examining how processing visual information affects motor control (dual-task loading) following ACLR.37,38
Given that efferent deficits have been reviewed comprehensively, a review examining afferent dysfunction following ACLR, and how it is measured, would help clinicians better assess and effectively target those deficits. Synthesising data from studies assessing ACLR somatosensory and visual system dysfunction is challenging due to the lack of studies and variety of outcome measures used, this paper therefore undertakes a scoping review to map key concepts and identify knowledge gaps.39,40
METHODS
The PRISMA guidelines for systematic reviews were followed with appropriate modifications for a scoping review.41
Research Questions
The original research questions were:
-
What differences exist within the somatosensory system between both ACLR and healthy controls, and between limbs in the ACLR population?
-
What differences exist within the visual system between both ACLR and healthy controls, and between limbs in the ACLR population?
-
What tests are used to measure the somatosensory and visual systems differences between ACLR and healthy controls?
Eligibility
The inclusion criteria for studies in the scoping review were: (1) at least one outcome measure which assessed somatosensory or visual sensory performance, (2) included subjects post ACLR, (3) published in English, and (4) full-text access. The studies could be of any design.39,40
Participants
Studies needed to include participants with unilateral ACLR. Participants were not excluded if they had concomitant knee injuries that required repair (such as meniscal damage). No restrictions were placed on ACLR technique or time from surgery. Studies were excluded if they included participants who had undergone revision ACLR.
Search Strategy
An electronic search was conducted in PubMed, SPORTDiscus, CINAHL, Medline and Embase in September 2021. No restrictions were placed on the date of publication. Two independent reviewers (TV and EK) conducted. The search related to the somatosensory system was (“ACLR” OR “ACL reconstruction” OR “anterior cruciate ligament reconstruction”) AND (“somatosensory” OR “proprioception” OR “somatosensation”)). The search related to the visual system was (“ACLR” OR “ACL reconstruction” OR “anterior cruciate ligament reconstruction”) AND (“visual” OR “visual-motor”).
Study Identification
The two reviewers (TV and EK) independently reviewed the titles and abstracts of the identified studies. If a study matched the eligibility criteria, the full text manuscripts were subsequently reviewed independently. The full reference list of identified studies was searched to locate relevant studies. Studies were downloaded to EndNote reference manager (https://www.endnote.com) and imported into Covidence software (www.covidence.org) to identify potential differences between reviewers and to reach agreement regarding study eligibility. Disagreements were resolved via discussion or third-party mediation (KM).
Data Extraction
Data were extracted by each reviewer (TV and EK) for all eligible studies, entered into spreadsheets, and combined. Disagreements were resolved via discussion or third-party mediation (KM). The standardized data extraction forms included details on the study design, participant details (age, time after surgery, surgical technique and percentage of the cohort being males), outcome measures, and results. To help with clarity of interpreting the results, the studies were sub-grouped based on the outcome measures utilized. For the somatosensory system results, studies were separated into those which assessed for central processing differences and those which assessed local somatosensory functions. The central processing studies were those that assessed for brain activity during tasks, which allows for interpretation of how information is processed in the central cortex. Local somatosensory functions were separated into studies that examined: proprioception (joint position sense), kinesthesia (threshold to detect motion) and other somatosensory functions (such as light touch and vibration). With regard to the visual system results, the studies were grouped into three categories: central processing, local visual function, and visual contribution to motor control. Central processing are those studies assessing how information is processed within the central cortex. Local visual function encompasses studies which utilized outcome measures that assessed visual functions, such as gaze tracking, visual memory and visual attention. Finally, studies were grouped into ‘visual contribution to motor control’ if their outcome measures assessed motor control during varying degrees of vision (to determine visual contribution) or with dual-cognitive tasks.
RESULTS
Outcome Measures
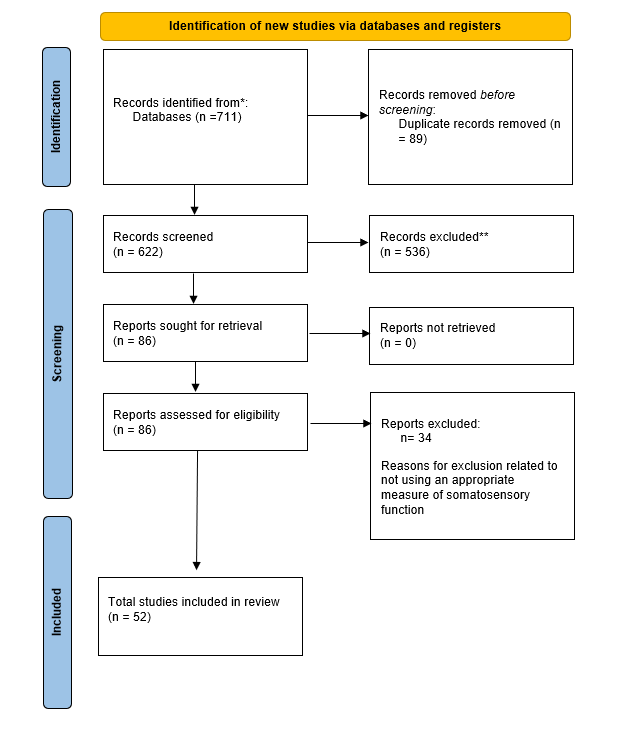
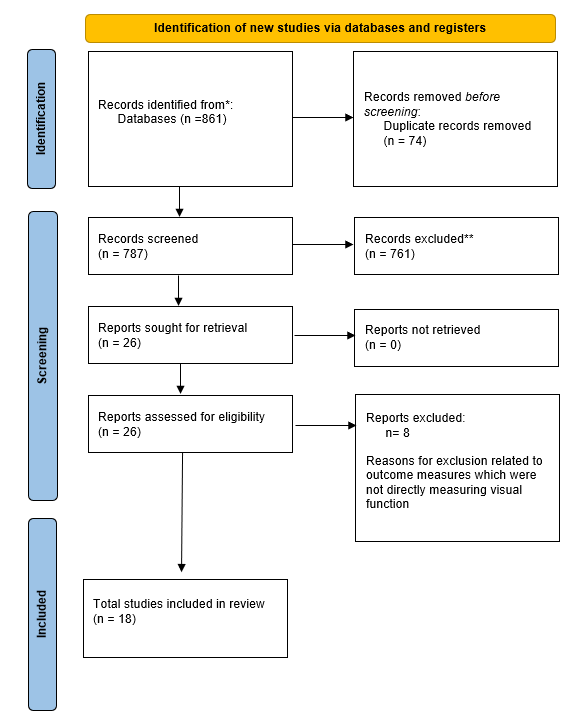
Seventy studies were included in this scoping review (Figure 3 and 4).


There was large heterogeneity of the outcome measures, so to assist readers the measures and their purpose are listed in Table 1 (somatosensory system) and Table 3 (visual system).
Somatosensory System
Fifty-two studies (see Tables 2, 3 and 4) were identified which assessed somatosensory function following ACLR. Nine studies examined central processing within the somatosensory system, while 44 examined local somatosensory functions (e.g proprioception, kinaesthesia and vibration). Some studies examined differences between the uninjured limb and ACLR limb (within-subject differences) (Table S1 in Supplementary information) whilst others compared the ACLR limb to a healthy control’s limb (between-group differences) (Table S2 in Supplementary information). Several papers examined both between-group and within-subject differences.
Central processing of somatosensory information
Of the nine studies that examined cortical processing, there was heterogeneity in the assessment methods: three studies utilised electroencephalogram (EEG), one utilised functional brain MRI, two utilised vibration perception threshold testing, two utilised posturography and one utilised light touch threshold detection testing. Whilst these techniques assess central processing, there are slight differences in the information obtained. EEG and functional brain MRI assess brain activity during simple motor tasks, with increased activity reflecting somatosensory dysfunction due to greater processing requirements. Posturography assesses postural control under varying circumstances to determine afferent system efficacy (e.g. vestibular, visual, somatosensory). Finally, vibration and light touch perception threshold testing examine central processing changes by comparing thresholds at sites local and distal to an injury. Increased perception thresholds at sites distal to the injury indicate central processing changes.
Six studies examined ACLR within-subject differences with the majority (4/6) demonstrating significant differences in somatosensory central processing (reduction in function).42–47 Two studies found increased EEG activity,42,46 and two posturography studies demonstrated reduced somatosensory function in the ACLR limb.43,44 However, both studies examining vibration perception threshold demonstrated no significant difference between limbs.45,47 Overall, studies suggest there are differences in central processing within the somatosensory systems in the ACLR limb, and vibration perception threshold may not be an appropriate method when examining ACLR within-subject differences.
Five studies examined somatosensory system central processing between ACLR participants and healthy controls, with all demonstrating significant differences.21,42,45,48,49 One study demonstrated increased vibration perception threshold in the ACLR limb both locally (around the knee) and globally compared to healthy controls.45 This study also demonstrated the uninjured limb of ACLR participants had increased vibration perception thresholds compared to healthy control limbs, further highlighting differences in the central processing of somatosensory information following ACLR. This was also reflected in a case control study48 in which light touch sensation at sites distal to the ACLR knee (medial malleolus and first metatarsal) was reduced as compared to healthy controls. The other two studies (EEG42 and functional brain MRI21) demonstrated increased somatosensory central cortex activity during simple motor tasks (non-weightbearing knee flexion and extension) compared to healthy controls.
Overall, following an ACLR, there are consistent differences in somatosensory system central processing. Not only does the ACLR limb have altered central processing as compared to the uninjured limb, but also as compared to healthy controls.
Local somatosensory function
Fifty studies examined various afferent pathways of somatosensory function: proprioception (joint position sense [JPS]), kinaesthesia (threshold to detect passive motion [TTDPM]) and vibration. The two most common were JPS and TTDPM, with large heterogeneity in the methods (Table 2).
Joint position sense
Twenty-seven studies examined within-subject JPS function (Table 2 and 3). Across the 27 studies a total of 35 outcomes were measured due to JPS being measured at multiple angles in some studies. Overall, there was mixed evidence with 13 studies demonstrating reduced JPS function in the ACLR limb, 20 demonstrating no significant difference and two demonstrating improved JPS function (Table 2). Participant demographics and time from surgery did not differ between studies with and without a difference. Time from surgery was quite varied across studies, ranging from four to 52.2 months. Of the studies that demonstrated a significant reduction in JPS function within-subject, the difference between the two limbs ranged from 0.8° to 3.8°.53,54,60
Twenty-five studies examined JPS function between the ACLR limb and healthy controls (Table 2 and 4). Across the 25 studies a total of 30 outcomes were measured due to JPS being measured at multiple angles in some studies. Similar to the within-subject studies, there were mixed findings, with 13 studies demonstrating significantly reduced JPS function in the ACLR group, 16 studies finding no significant difference and only one reporting improved JPS function in ACLRs.79 Of the studies that demonstrated a significant reduction in JPS function between ACLR limbs and healthy controls, the JPS difference between limbs ranged from 0.4° to 5°.57,60,78
The small differences and the similar number of papers identifying JPS performance as being negatively affected as those reporting no difference for both between-group and within-subject differences, highlights the difficulty in measuring this variable. However, with almost 50% of the identified studies demonstrating reduction in proprioceptive function, JPS should be routinely assessed in ACLRs post-surgery. The small differences between-group and within-subject makes it difficult for clinicians to reliably monitor changes over time. Also, large heterogeneity in outcome measures and lack of reporting of the standard error of measurement makes it hard to draw firm conclusions. Future research should report the reliability and standard error of measurement values for the outcome measures utilised to help readers and clinicians interpret the findings better.
Threshold to detect passive motion (TTDPM)
Seventeen studies examined within-subject TTDPM performance (Table 2 and 3), with mixed findings. Across the 17 studies a total of 20 outcomes were reported due to some studies having multiple outcome measures. Nine studies reported reduced ACLR limb TTDPM (from 0.2° to 1.4°),45,54 while eleven studies demonstrated no significant difference.
Thirteen studies examined TTDPM performance between the ACLR limb and healthy controls (Table 2 and 4), again with mixed findings. Five studies reported significantly reduced ACLR limb function, while seven studies reported no significant difference. One study reported significantly better ACLR function. Of the studies that demonstrated a significant reduction in TTDPM performance between ACLR limbs and healthy controls, the JPS difference between limbs ranged from 0.3° to 2.8°.45,91
Akin to JPS studies, a similar number of papers for both between-group and within-subject differences identified TTDPM performance as being negatively affected as those reporting no significant difference. In addition, the differences are also small. This may suggest that TTDPM is a function that should be routinely assessed in ACLRs as it may be negatively affected but that it is a variable that would be hard for clinicians to monitor for recovery due to the small magnitude in the differences. Also, there is large heterogeneity in testing methodology with limited reporting on standard error of measurement for each outcome measure which makes firm conclusions difficult.
Other afferent components of local somatosensory function
Other measures of somatosensory function can include vibration perception threshold testing (of local sites around the knee). However, only two studies examined this, with conflicting findings. Courtney et al45 found significantly greater perception thresholds in the ACLR limb compared with both the uninjured limb and healthy controls, while Blackburn et al47 reported no significant difference between the ACLR limb and the uninjured limb. Greater vibration perception thresholds around the knee can indicate local negative changes within the somatosensory system. The lack of research in this area makes it difficult to make firm conclusions regarding the potential effect of ACLR on this somatosensory function.
Visual System Results
Eighteen studies (Table 6) assessed visual system differences following ACLR. Across the 18 studies a total of 20 outcomes were reported due to some studies having multiple outcomes measures. Fifteen studies examined differences between ACLR participants and healthy controls, whilst five studies examined differences between limbs in the ACLR participants. The studies identified assessed specific visual processes (both local and central) and/or the contribution of the visual system during motor control.
Central processing
Six studies21,35,83,99–101 assessed differences in visual system central processing between ACLR participants and healthy controls. No studies assessed within-subject differences in the ACLR population. Five of the six studies21,35,83,100,101 demonstrated increased activity in visual processing regions of the brain, via either functional brain MRI or EEG, in ACLR participants during simple movements (Z-max scores of greater than 4). Increased activity may be a sign of compensation with regards to altered somatosensory information or a sign of dysfunction within the visual system.24,36 These studies were completed over a large time range post-surgery (1.5 ± 0.2 months101 to 43.3 ± 33.3 months100). This may indicate that differences in visual processing activity are persistent and may develop quite early post-surgery. The remaining study demonstrated no significant difference.99 Various visual processing areas within the brain have been identified as areas of greater activity within the ACLR population. Grooms and colleagues21 demonstrated significantly greater activation of the lingual gyrus, which is responsible for visual processing and visual memory, suggesting a compensatory mechanism for reduced somatosensory information described earlier (somatosensory results). The results from Criss and colleagues100 further supports this. They found increased activation of regions responsible for visual processing and combined visuospatial perception and attention.
Overall, there are differences in ACLR visual system central processing. It is unknown if these differences are present prior to ACLR or if it is a result of ACLR. Future prospective studies (assessment pre-ACL injury and then post-ACLR) are required to determine this.
Local visual function
Six studies examined local visual function differences between ACLR participants and healthy controls with conflicting results.37,38,76,83,102 One study38 assessed local visual function with multiple outcome measures, so there is some overlapping of results. There are numerous methods to assessing local visual function including computer-based visual memory tasks,83 gaze tracking37 and measuring reaction times to visual stimuli38 (Table 3). Three studies37,76,102 demonstrated ACLR significantly reduced local visual function (related to gaze tracking of multiple objects, visual attention and reaction to visual stimulus) , three studies37,38,83 demonstrated no significant difference (related to visual memory, gaze tracking stationary object and reaction time to visual stimulus), and one study38 demonstrated ACLR improved function (related to visual attention) . The contrasting findings may be due, at least in part, to the large heterogeneity in outcome measures (table 5). Some studies utilised neurocognitive tests to assess visual attention (the ability to select specific objects in the environment and filter out the irrelevant information) and visual memory (the ability to store and recall visual information,83 whilst others utilised tests to assess the qualities of vision such as gaze tracking (ability to track objects in the environment)37 and reactions to visual stimulus.38,76,102 Bodkin and colleagues37 found that their ACLR group had large differences (Cohen d= 0.96) when tasked with tracking a moving object, resulting in a greater number of visual gaze errors, but no differences when focusing on a stationary object. This contrasting finding has significant relevance when playing sport. ACLR are also slower to react to visual information and adjust their posture accordingly.76 With the majority of ACL injuries being non-contact in nature and heavily influenced by movement strategy,103,104 the changes to visual information processing in ACLRs may influence their motor strategy with consequences for performance and re-injury susceptibility.
Only one study102 assessed within-subject differences in local visual function demonstrated reduced function. Roelofsen et al102 assessed the effect of visual feedback on leg amplitude movement during a visual tracking task. They demonstrated that ACLRs had significantly decreased leg amplitude in response to visual feedback in comparison to not only healthy controls but also to their limb prior to surgery. This result may indicate that there are changes in the way visual information is processed but they may also be the result of reduced proprioception.
Visual contribution to motor control
Nine studies44,83,102,105–110 examined the contribution of vision to motor control in ACLR population as compared to healthy controls, with six44,83,102,106,109,110 finding ACLR had increased contribution . During both postural and movement tasks, visual reliance was determined by a participants’ balance and movement control worsening, respectively, with the removal or alteration of visual input. Contrastingly, four studies105–108 reported no significant difference. This conflict may be due to large heterogeneity in testing methodologies and data analysis techniques. A systematic review with meta-analysis105 demonstrated no significant difference between ACLRs and healthy controls in their performance during a single leg postural control task which compared eyes open to eyes closed; both groups experienced similar declines in performance when their vision was blinded (ACLR= 42.9% decline versus controls= 44.4% decline). The studies included in this meta-analysis used traditional centre of pressure metrics (path, amplitude, and calculated stability indexes). However, posturography and frequency analysis during double leg standing utilised in three studies demonstrated increased reliance on the visual system (via assessment of ultra-low frequencies) in the ACLR population as compared to healthy controls.44,110,111 This was further support by Chaput et al83 who demonstrated higher performance on a visual motor subscale in a neurocognitive test was strongly associated with better time-to-stability performance during a jump-landing task (r= -0.61, p=0.03) in an ACLR population, whilst no such association was found in healthy controls.83
Four studies102,108,111,112 examined within-subject differences in the ACLR vision contribution to motor control with mixed findings. Two studies102,111 demonstrated significant reductions in posturography111 and leg positioning task102 performance whilst two studies108,112 demonstrated no significant difference during a change of direction112 and hopping108 task. The two studies102,111 demonstrating significant differences compared the ACLR limb post-surgery to the limb prior to surgery, while the two studies108,112 demonstrating no significant difference examined differences between the ACLR limb and uninjured limb, potentially indicating that individuals become more reliant on visual information following ACLR. The two studies108,112 which demonstrated no significant difference utilised functional tests such as hop for distance (blinded versus full vision)108 and a change of direction (full vision versus disrupted vision)112 while the two studies102,111 demonstrating a difference utilized tests requiring small adjustments in posture. This may suggest that whole-body functional tasks could allow for compensatory movements from other body segments which mask the altered motor control within the ACLR limb.
DISCUSSION
The aim of this scoping review was to summarize any differences in somatosensory and visual systems following ACLR. The results identified both within-subject and between-group differences in central processing (somatosensory and visual systems) in the ACLR cohort which may represent sensorimotor dysfunction. However, when assessing somatosensory functions (such as JPS and TTDPM) and the visual system (processing central and local visual information, and the contribution of vision on motor control) there were mixed findings with a tendency for between-group (ACLR versus healthy controls) differences to be present.
Changes That Occur in the Somatosensory and Visual Systems Following ACLR
Previous reviews have focused on the negative efferent changes within the sensorimotor system following ACLR which have been hypothesized to occur in response to dysfunction within the afferent pathways.24 It has also been hypothesized that an over reliance on the visual system to maintain postural control and execute movements may develop in response to dysfunction within the somatosensory system.6 The results of this review confirm that there are significant differences between the afferent pathways, both somatosensory and visual, of ACLR participants and healthy controls, and also between limbs in the ACLR cohort with studies assessing central processing demonstrating alterations in somatosensory processing and increased activity in the visual system.21,100,115 However, it is not possible to determine if the differences are a reflection of dysfunction that occurs as a result of the ACLR surgery or is present prior to surgery due to the lack of prospective research available.
As previously mentioned, the ACL is highly innervated with mechanoreceptors with damage leading to a reduction in somatosensory functions such as proprioception and kinaesthesia.10,11 However, somatosensory functions are thought to improve once the afferent fibers regrow into the ACL graft over the following three to six months.31 This review supports the notion of a reduction in proprioception59,67,96 and kinaesthesia45,91,92 in the ACLR limb as compared to the participants’ uninjured limb. While some of these findings were reported for participants who were less than six months post-surgery, there was an almost equal number of studies which demonstrated persistent reduced function in participants whose ACLR graft should have been reinnervated (36 to 64 months post-surgery).52,53,56,57 The persistent reduced function could indicate that some individuals do not experience reinnervation of their graft.116 Another more likely explanation is that these participants have ongoing dysfunction in central processing of the somatosensory information, as evidenced by the functional brain MRI and EEG studies,21,42,44,46,49 despite having received rehabilitation.
Motor control requires the afferent systems to continuously obtain information regarding the body and its position within the environment so that appropriate motor responses can be made to account for any perturbations.117–119 Dysfunction within the somatosensory system may result in greater reliance being placed on the other afferent systems such as the visual system to obtain information from the environment. This has been previously shown in injuries, such as chronic ankle instability.120 The results of this review appear to support the notion that increased reliance on the visual system also occurs in the ACLR cohort. Four studies utilizing methods to assess central processing in the visual centers demonstrated greater activity in these centers as compared to healthy controls during simple motor tasks.21,35,98,100,113 It has previously been suggested that increased reliance on the visual system may increase the risk of sustaining a primary ACL injury, potentially as a result of the athlete either missing environmental cues or reacting slowly to a stimulus, thereby executing a movement with poorer technique.121 Therefore, increased reliance on the visual system identified in individuals following ACLR may have an implication for increased risk of second ACL injury.35 Bodkin et al37 reported that ACLR participants exhibited significantly greater visual gaze errors as compared to healthy controls when tracking a moving target. The findings may provide some support for the notion of ACLRs being more visually reliant as they found it harder to track a moving target, although it may also represent that this population has poorer visual function, which is pertinent for picking up cues in a chaotic environment which is encountered is most field-based sports. The findings were supported by Armitano-Lago et al76 who reported that ACLR participants responded more slowly to a visual stimulus than healthy controls when tasked with making a postural adjustment. Slower reaction times were seen in the ACLR group when performing a stepping task but not so when completing a task whilst seated, suggesting that as task complexity increases, then individuals with dysfunction within motor planning and execution cortical areas will begin to demonstrate differences.
A Reflection on Assessing Somatosensory and Visual Dysfunction
Although differences have been found to exist in the somatosensory and visual systems following ACLR, a common issue for clinicians is having the tools to identify this dysfunction in their athletes. Central processing changes are identifiable via methods such as functional brain MRI and EEG. However, both methods are not feasible for many clinicians due to the cost and lack of access to the technology. An alternative approach to identifying somatosensory dysfunction may be possible by identifying JPS or TTDPM deficits in athletes greater than six months post-surgery. The most appropriate method to measure JPS would be image-calculated angulation because most clinicians do not have access to isokinetic dynamometers. However, very few studies have published the reliability of the outcome measures they used which can make it difficult for clinicians to utilise in clinical practice. One study96 which utilized image-calculated angulation to measure JPS published the reliability (ICC= 0.86-0.92) and minimal detectable change (1.3° to 2.4°) for their testing methodology,122 therefore allowing it to easily be employed in clinical practice. With regards to TTDPM, there are a limited number of methods to assess TTDPM without using isokinetic dynamometers. Hence, more research is required to find reliable methods to assess TTDPM that are also easy for clinicians to employ within their clinics. So, the reality for clinicians is that deficits likely occur in some, if not all, individuals following ACLR. However, they are unlikely to be able to assess these deficits in the clinic, so clinicians should consider employing exercises which redevelop these qualities.
With regards to assessing the visual system, there was again large heterogeneity in the outcome measures used. This is especially evident in the variety of outcome measures used to assess local visual processing function (e.g. trail making test, gaze tracking and neurocognitive testing). Whilst there may be differences identified in gaze tracking37 or trail making tests,38 it is still not clear what impact this has on the ACLR cohort with regards to risk of reinjury or sporting performance. More prospective research is needed to identify the attributes of visual processing that are most pertinent for athletes following ACLR to minimise the risk of reinjury and to return to preinjury performance levels. Previous research has identified visual memory, processing speed and reaction times on a neurocognitive test as factors associated with greater risk sustaining a primary ACL injury.121 The greater availability of sensory stations123 (mobile tablet technologies with preloaded visual assessments) which assess these factors plus a number of other local visual processing attributes may make it easier for not only clinicians to assess athletes with a single tool but also for researchers to have a consistent outcome measure to measure athletes for prospective studies. When assessing the effect of vision on movement control, posturography with analysis of frequencies currently appears to be a consistent method to identify if there is an over-reliance on the visual system during static tasks110,111 but it may not be feasible for clinicians as there are only a few commercially available systems. In summary, visual reliance most likely exists along with some dysfunction of visual processing in the ACLR population but methods of measurement are limited for clinicians. Clinicians should look to include training modalities that improve visual processing.
Clinical Implications for Rehabilitation
Current ACLR rehabilitation programs follow a common path of: (1) regaining range of motion and control of the knee, (2) strength and hypertrophy training, (3) plyometric training, (4) running (linear and multi-directional) and (5) sports-specific drills.124–126 Alongside the structured rehabilitation program, athletes go through a process of gradual reintroduction to training in the sport itself prior to a reintroduction to competition. However, much of the literature which identified dysfunction within the central processing of somatosensory21,42,49 and visual information21,100 was conducted in patients who had already completed rehabilitation (although the specific makeup of their rehabilitation programs was not reported) and returned to sport (average time from surgery ranged between 12 and 48 months). If the participants had completed rehabilitation that would be expected as standard care, then this continued dysfunction could suggest that there is a missing element in either current rehabilitation programs or the long-term follow up care of athletes. Hence, future research is required to identify (1) methods applicable to a clinical setting to identify individuals with a deficit and then (2) methods to reduce the reliance on the visual system.
Along with identifying methods to reduce visual reliance, knowing when to implement these methods is important as well. Proprioception deficits have been identified within the first four weeks following ACLR,91 and Lehmann et al113 have also demonstrated that increased reliance on the visual system (at the central processing level) may begin within six weeks following ACLR. The results suggest that clinicians aiming to reduce reliance on the visual system need to implement interventions very soon post-operatively. Therefore, future research should aim to identify effective methods to reduce reliance on the visual system.
Limitations
There are several limitations to this scoping review. Firstly, much of the research identified was retrospective in nature meaning that it is not possible to determine if any of the identified somatosensory and visual dysfunction in the ACLR cohort was present prior to the injury or prior to the ACLR. Secondly, no critical appraisal of the studies was performed due to the small number of studies in area of somatosensory and visual dysfunction, so threats of bias were not identified within the selected studies, and this may affect the results obtained. However, because visual dysfunction is quite a new area of research in the ACLR literature, the decision was made to include all available studies so that trends could be observed. As this area of science matures, then future studies could be more selective in the quality of studies that they use for review. Furthermore, the review predominantly examines somatosensory and visual variables but not how it relates to patient outcomes. Future research should assess how these variables are associated to patient outcomes. Another limitation was that there were several studies utilizing participants who were greater than two years post-ACLR. This may potentially introduce confounders to the results as the participants had been discharged from rehabilitation and returned to general activity. Therefore, it is unknown what influence returning to general activity may have on afferent function. Lastly, the reliability of a number of the outcome measures used in the selected studies were not reported, making it difficult to confidently trust the statistical and clinical significance of the differences observed.
CONCLUSION
This scoping review highlights the within-subject (ACLR limb vs uninjured limb) and between-group (ACLR versus healthy controls) differences within the somatosensory and visual systems. The evidence highlighting differences in central processing of the somatosensory and visual systems demonstrates the potential impact that ACL injury and/or ACLR has on individuals. Within the somatosensory system, reduced proprioceptive and kinesthetic function has been demonstrated in the ACLR limb as compared to the contralateral uninjured limb. Similarly, the ACLR limb has reduced proprioceptive and kinesthetic function as compared to healthy controls. Increased reliance on the visual system occurs in response to somatosensory dysfunction as evidenced by altered central processing, potentially resulting in errors in visual processing and adversely affecting motor control.
Future large-scale studies are required to examine if there are differences in visual processing between athletes following ACLR and healthy controls. Similarly, more research is required to examine the effect of visual reliance on biomechanics and the effectiveness of interventions in treating these dysfunctions as well.
Funding
No funding was received for the completion of the study.
Conflicts of interest
No conflicts of interest exist for the authors.
Acknowledgments
The authors would like to Luis Arias for producing the illustrations for the study.