INTRODUCTION
Injury to the anterior cruciate ligament (ACL) and subsequent reconstruction (ACLR) can be associated with a multitude of negative outcomes including decreased physical activity,1–3 decreased health-related quality of life (HRQL)4 and earlier development of osteoarthritis5,6 for some patients. Systematic reviews with meta-analyses have revealed that ACLR is associated with the development of osteoarthritis5,6 and prevalence estimates are as high as 36% as soon as 10-years after reconstruction.7 Typically, once a patient undergoes ACLR and completes formal rehabilitation, they are no longer under the direct care of a physician until early osteoarthritis symptoms have developed. By the time a patient presents to their provider with clinical signs and radiographic evidence of arthritic changes, the damage to the joint is irreversible.8 Given the nature of the development and presentation of osteoarthritis, clinicians and researchers alike have aimed to identify assessments that can classify individuals as symptomatic or non-symptomatic early on in their disease progression.9 The ability to identify patients that are symptomatic before the visualization of radiographic changes is pertinent for the advancement of intervention strategies to delay osteoarthritis development.9
The Englund classification system was originally developed to identify patients with a history of meniscectomy who had symptomatic knees associated with osteoarthritis development.10 Specifically, the Englund classification classifies patients with symptomatic knees if they have a score of ≤87.5 on the Knee Osteoarthritis Outcome Score (KOOS) Quality of Life subscale, and two or more of the following scores on the remaining subscales: ≤86.1 on the KOOS-Pain, ≤85.7 on the KOOS-Symptoms, ≤ 86.8 on the KOOS-Activities of Daily Living (ADL) and ≤85.0 on the KOOS-Sports and Recreation (Sports) subscale.10 The Englund classification has also been applied to patients early after ACLR.11,12 Recent investigations have explored the relationship between symptomatic knees and clinical outcomes,12 and explored the utilization of these criteria in patients approximately 6-months post-ACLR.11 However, to the authors’ knowledge, there is limited evidence that has explored the relationship between osteoarthritis symptomology, health-related quality of life and psychological outcomes in people with a history of ACLR.
Deficits in HRQL and fear-avoidance beliefs in people with a history of ACLR have been identified compared to healthy controls.13 However, there is a lack of evidence to suggest these outcomes are different between people that are classified by the Englund criteria as symptomatic or non-symptomatic.10 Understanding this relationship is important as clinicians and researchers begin to focus on the development of holistic patient-centered treatment strategies to address pain, symptoms and osteoarthritis in people with a history of ACLR. In addition, physical activity is a part of the non-surgical treatment strategy for osteoarthritis.14 Therefore, it is important to examine psychological outcomes that may influence physical activity participation in this population such as fear-avoidance beliefs and resilience. Fear- avoidance beliefs have been associated with physical activity after ACLR.4,15 Resilience is a term often used to describe a person’s ability to adapt and overcome to their circumstances.16 Factors associated with resilience such as communication and social support, self-efficacy and goal setting have been previously examined in patients who successfully undergo ACLR.17 Previous literature has determined that patients with knee osteoarthritis with high resilience had a higher odds of having better self-reported overall health.18 Therefore, the purpose of this study was to examine differences in HRQL and psychological outcomes in symptomatic and non-symptomatic individuals with a history of ACLR, as classified by the Englund criteria.10 It was hypothesized that there would be significant differences in HRQL and psychological outcomes between these two groups. Specifically, we hypothesize that participants classified as symptomatic will have lower HRQL, increased fear-avoidance beliefs and decreased resilience compared to participants classified as non-symptomatic. These results will further support the need to develop treatment algorithms that can effectively address HRQL and psychological outcomes in people with a history of ACLR that have symptomatic knees.
METHODS
Study Design
A cross-sectional survey-study was used to examine differences in patient-reported outcomes between participants with a history of ACLR with symptomatic knees and those without symptomatic knees. The dependent variables were scores on the Tegner Activity Scale, the Brief Resilience Scale (BRS), the modified Disablement in the Physically Active Scale (mDPA), and the Fear-Avoidance Belief Questionnaire (FABQ).
Participants
Participants with a history of ACLR were recruited via ResearchMatch. ResearchMatch is a national health volunteer registry that was created by several academic institutions and supported by the U.S. National Institutes of Health as part of the Clinical Translational Science Award (CTSA) Program.19 To be included, participants must have been between the ages of 18-40 years, had a history of a unilateral or bilateral ACLR within the prior 10 years and had been cleared to participate in physical activity by a physician. Participants were excluded if they had surgery to the lower extremity within the last year, reported any additional ligament repair at the time of ACLR surgery, had a lower extremity injury within the prior six weeks, were diagnosed with any condition that may affect their ability to participate in physical activity, or were unable to speak or read English. This study was approved by the University of Kentucky Institutional Review Board.
Procedures
Participant recruitment occurred from July 2020 to December 2020. Interested participants received a link via email to participate that first included an electronic consent form. If the participant agreed to participate, they clicked “yes” on the electronic consent form, and proceeded to the anonymous survey. Next, the participants completed an inclusionary form to ensure all participants met the inclusion criteria followed by a demographic questionnaire that recorded age, race, sex, ethnicity, physical activity participation, and lower extremity injury history information. Included in this questionnaire, participants recorded details of their ACLR(s) such as graft type, post-operative bracing, and post-operative rehabilitation participation and years since their most recent ACLR. Each participant then completed the patient-reported outcomes. The patient-reported outcomes were not administered in a randomized order. All data were collected utilizing Real Electronic Data Capture (REDCap).20,21
Instrumentation
The Tegner Activity Scale: The Tegner Activity Scale was utilized to determine participants’ activity level prior to their knee injury and after their knee injury. From these data, an activity change score was calculated by subtracting their previous activity level from their current activity level. A negative value indicates a decrease in activity level after their injury, a positive value indicates an increase in activity level after their injury. The Tegner is a reliable measure of self-reported physical activity in patients with a history of ACLR.22 Recent analyses revealed acceptable test-retest reliability and a minimal detectable change of one point in patients that had recently undergone ACLR.22
The Brief Resilience Scale: The 6-item Brief Resilience Scale (BRS) was used to measure self-reported resilience. Questions 1,3 and 5 were assessed on a 5-point Likert Scale with 1 meaning “strongly disagree” and 5 meaning “strongly agree”.23,24 Questions 2,4, and 6 were reversed scored and assessed on a 5-point Likert Scale with 1 meaning “strongly agree” and 5 meaning “strongly disagree”.23,24 The final scores are interpreted as 1.00-2.99 low resilience, 3.00-4.30 normal resilience, and 4.30-5.00 high resilience.24 The BRS has acceptable test-retest reliability and internal consistency in healthy populations and populations with various health conditions.24
The Modified Disablement in the Physically Active Scale: The mDPA was used to measure general HRQL. The mDPA consists of two summary components that comprise the original DPA, the Physical summary component (PSC) and the Mental summary component (MSC).25 The 12-item mDPA-PSC and 4-item mDPA-MSC are scored on a 5-point Likert scale with 0 representing “no problem” and 4 representing a “severe problem.” The scores for each subscale are summed, and a higher overall score indicates a higher level of disablement.25 The original DPA has acceptable test-retest reliability, internal consistency and validity for people with a history of injury, acute injury and individuals classified as healthy.26 The mDPA has excellent internal consistency.25
Fear Avoidance Beliefs Questionnaire: The FABQ modified for the knee and sports is a 15-item instrument that was used to measure fear-avoidance beliefs. The original FABQ consisted of two subscales, physical activity (PA) and work,27 but has since been modified for patients with knee injury by changing the word “back” to the word “knee”28 and for sports where the word “work” was changed to “sport”.29 The 5-item FABQ-PA subscale and 10-item FABQ-Sports subscale are scored on a 7-point Likert scale where 0 indicates “completely disagree” and 6 indicates “completely agree.” Higher scores for each subscale indicates higher fear avoidance beliefs.27 The original FABQ has acceptable test retest reliability and internal consistency for both subscales in patients with chronic low back pain.27
Knee Injury and Osteoarthritis Outcomes Score : The KOOS was used to measure self-reported knee function and classify the participants as symptomatic or non-symptomatic according to the Englund symptomatic knee classification.10 The 42-item KOOS evaluates five dimensions regarding knee function: pain (KOOS-Pain), current symptoms (KOOS-Symptoms), activities of daily living (KOOS-ADL), function in sports activities (KOOS-Sports), and quality of life (KOOS-QOL) relating to the knee.30 A 5-point Likert Scale is use to score the separate subscales.30 The highest possible score on each subscale is 100 with higher scores indicating higher function.30 In order to be classified as symptomatic, participants had to score ≤ 87.5 on the KOOS-QOL, and score below the following cut-offs on two or more of the remaining subscales: ≤ 86.1 on KOOS-Pain, ≤ 85.7 on KOOS-Symptoms, ≤ 86.8 on KOOS-ADL, and ≤ 85 on KOOS-Sports.10 All five subscales have demonstrated acceptable internal consistency and test retest reliability in athletes with a history of ACLR31 and many other patient populations with knee injuries and osteoarthritis.32
Statistical Analysis
Descriptive statistics (means and standard deviations) were calculated for participant demographics. If an instrument was missing a response to an item, the person mean was calculated for that specific scale and inserted for the missing data point. The outcome data were not normally distributed and thus summarized using median and interquartile ranges (IQR). Due to the non-normal distribution of the data, independent-samples Mann-Whitney U tests were used to examine differences in the demographic variables and patient-reported outcomes between those participants categorized with symptomatic knees and those classified with asymptomatic knees. Alpha was set a-prior to p<0.05. All statistical analyses were performed in IBM SPSS Statistics Processer version 28.0.0.0.
RESULTS
There were a total of 29 participants, 17 (3 females) were classified as participants with symptomatic knees and 12 (7 females) classified as non-symptomatic knees. A total of five participants classified in the symptomatic knee group had a history of two ACLRs, while none of the participants classified in the non-symptomatic knee group had a history of more than one ACLR. Summaries of the demographic variables can be found in Table 1. Participants with symptomatic knees had a significantly higher BMI than participants with non-symptomatic knees (p=0.021).
Summaries of the dependent variables for each group can be found in Table 2. Participants in the symptomatic group had worse HRQL as measured by the mDPA-PSC (<0.001) and mDPA-MSC (p=0.018), higher levels of fear-avoidance beliefs (FABQ-PA: p<0.001. FABQ-Sport: p=.001), and lower levels of resilience compared to those participants in the non-symptomatic group (p=0.030, Table 2). There were no differences in current physical activity or change in physical activity levels between the two groups (Table 2).
DISCUSSION
The purpose of this study was to examine differences in HRQL and psychological outcomes in participants with a history of ACLR that were classified as symptomatic compared to those classified as non-symptomatic according to the Englund criteria.10 The hypothesis was confirmed as participants with symptomatic knees had lower HRQL, higher fear-avoidance beliefs and lower resilience compared to the non-symptomatic group. Furthermore, the authors identified differences in BMI between groups, with participants with symptomatic knees having a higher BMI than those with non-symptomatic knees. While these differences identified are not causal, and are limited in their application based on study design, these results are foundational to the development of effective intervention strategies to address osteoarthritis symptomology in people with a history of ACLR.
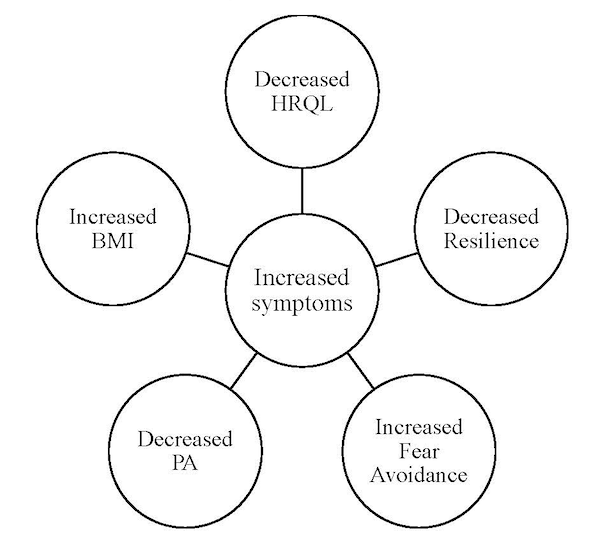
The results of this cross-sectional analysis present an interesting, potential cyclical cascade of outcomes that are of primary concern for the long-term health of patients with a history of ACLR as presented in Figure 1. The results of this study align with previous research demonstrating decreased HRQL after knee surgery33 and in individuals with symptomatic knees.34 While the authors did not attempt to quantify specific symptoms in this sample, previous studies have identified that knee pain, stiffness, and weakness in surrounding musculature are common in those with symptomatic knees.34 It is likely that changes in knee symptoms negatively impact other aspects of life as previous literature has identified links between HRQL, BMI, and physical activity participation. For example, individuals with symptomatic knees after ACLR often present with increased BMI34 which align with the results of the present study. Additionally, higher BMI has been associated with decreased HRQL in the general population,35 adolescent populations,36 and older adults (>65 years).37 However, based on the study design, it is unable to be determined whether those with symptomatic knees had higher BMI at time of injury or surgery or whether these differences are associated with factors experienced between ACLR and participation in this study.
Individuals with symptomatic knees also reported increased fear avoidance beliefs compared to individuals with non-symptomatic knees. Fear avoidance refers to the avoidance of activities that could illicit pain, potentially cause reinjury, or any other negative stimuli.38 The Fear Avoidance Model suggests that increased perceptions of fear and increased incidence of avoidance will lead to disuse, dysfunction, and depression.39 Similarly, pain catastrophizing, kinesiophobia15 and fear of reinjury40,41 are common psychological factors that have been observed post-ACLR. Qualitative evidence demonstrates that fear of reinjury is a primary barrier for returning to activity after ACLR and many patients self-limit and/or avoid physical activities to avoid reinjury.40,41 We did not identify significant differences in physical activity measured by current Tegner scores between our two groups; however, we did see that the symptomatic participants scored one point lower on the Tegner activity scale than the group that had non-symptomatic knees and had a larger change from baseline. While we are not able to report differences in physical activity between the groups or a cause-and-effect relationship between ACLR, decreased HRQL, higher BMI and decreased activity, we do believe that these findings are of interest for future research investigations. Fear-avoidance beliefs have been associated previously with physical activity in people with a history of ACLR.4 Individuals with a history of ACLR participate in less MVPA compared to non-injured peers.2 This is problematic as physical activity has been found to be the most effective intervention for treating pain in patient with knee osteoarthritis,42 and is known to be beneficial for weight loss,43 potentially decreasing a person’s BMI. Additionally, it has been demonstrated that individuals who participate in greater MVPA report higher HRQL even when they report increased knee symptomology.44 Lastly, it is also important to note that all 5 participants that reported having a history of 2 ACLR were included in the symptomatic group.
Finally, the symptomatic group demonstrated lower resilience scores compared to the non-symptomatic group. Resilience, as operationally defined by Liu et al.,16 is the process by which an individual adjusts and responds to challenges. Resilience has been sparsely examined as a psychological factor associated with outcomes after ACLR; however, qualitative evidence has identified resilience as a key theme.45 Johnson et al. concluded that patients that were more resilient had better outcomes after ACLR,17 while Disantis et al.46 revealed that individuals that viewed recovery as an opportunity to ‘overcome adversity’ experienced personal growth as a result of their injury. It has been suggested that cognitive behavioral therapies and resilience training can improve coping strategies and decrease psychological distress in patients undergoing knee surgery.47 This, in turn, may have positive effects on other psychological factors (e.g., fear avoidance), physical activity adherence, and HRQOL (Figure 1).

Limitations
This study was not without limitations. All data associated with this investigation are self-reported and were captured via electronic survey. Participants may not have understood every question presented and were not able to ask clarifying questions based on this study design. Methods used for patient classification were also limited to patient self-reports. No additional clinical criteria (i.e., radiographs) associated with the determination of a symptomatic knee were used, other than the completion of the KOOS survey. It is possible that the symptoms identified by completion of the KOOS could have been from origins other than osteoarthritis. Furthermore, the results of this study cannot be considered evidence of a cause and effect relationship. This was a cross-sectional study design that was only able to determine differences between the two groups of participants. These results are preliminary in nature, and are intended to support future investigations to determine the progression of osteoarthritis symptoms, quality of life, physical activity and fear-avoidance beliefs. Given the cross-sectional nature of this investigation, we are unable to determine if these outcomes preceded the ACL injury, reconstruction, and now symptomatic knee. The authors are also unable to determine if participants underwent any other lower extremity surgery after their ACLR but within the inclusionary time frame. Future investigations into the development of these outcomes should be longitudinal in nature to better understand the cascade of events. Lastly, these data were captured during COVID-19 in a small sample. It is possible that restrictions associated with the pandemic could have impacted participant responses on the surveys and responder bias may have influenced those who chose to complete the survey.
CONCLUSION
In conclusion, differences in BMI, HRQL, fear-avoidance beliefs and resilience were identified between participants with symptomatic knees and those with non-symptomatic knees. This series of relationships may be a cascade of events that can negatively impact health outcomes across the lifespan for this post-ACLR population. It is necessary for future longitudinal investigations to examine these outcomes after ACLR and as these individuals progress after rehabilitation and beyond clearance from formal rehabilitation. Should it be warranted, clinicians may consider patient education with a focus on the importance of physical activity for decreasing pain and other symptoms associated with symptomatic knees. Clinicians may consider exercise as a prescription for symptomatic joints after injury, but must include an overall assessment of the patient’s psychological variables (e.g. fear-avoidance beliefs and resilience) and consider additional treatment strategies as warranted.
Acknowledgements
This project was supported by NIH CTSA UL1TR01998.
Conflicts of interest
The authors report no conflicts of interest.