
INTRODUCTION
Team handball is an Olympic sport, and it is known for its complexity of high technical demands in both the lower and upper extremities, together with high speed and physical contact. Repeated throws are primarily performed with the hand above shoulder height with maximal and submaximal throwing velocity. The shoulder-specific loads vary with the total number of throws, playing position, and type of training, and shoulder pain is one of the most common injuries.1,2 Shoulder pain affects athletes’ performance, training, and daily life.3–5 In Norway, 44–75% of all senior handball players have experienced shoulder pain at some point, and 12–40% were still participating in training and matches, but with modifications.4,6 Several authors have identified deficits in glenohumeral range of motion, strength imbalances, increasing training load, and scapular dyskinesis as risk factors for developing shoulder pain in adolescents and senior elite team handball players.7–10 With the high prevalence and persistence of shoulder pain in adolescents and senior elite handball players, there is a need for high-quality assessment tools to evaluate upper-body strength and stability. A clinical assessment tool should be easy to implement in the field and at a low cost, but most importantly, it should be a tool that could assist the coach, athlete, and medical team in discerning injury risk and return to play for athletes with and without a history of shoulder injury. Several sport-specific functional tests are presented in the literature to assess performance in throwing athletes. Even though the tests do not include throwing, they involve the entire kinetic chain in the test performance: the Posterior Shoulder Endurance Test (PSET),11 the Shoulder Endurance Test (SET),12 the Y-Balance Test for upper extremities,13 the seated medicine-ball throw,14 and the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST).5,15–18
The CKCUEST was originally described by Goldbeck and Davies19 to provide objective data on muscle capacity and neuromuscular control that could assist the clinician in determining the patient’s readiness to return to activities, resume competition, or continue further rehabilitation. The CKCUEST requires the proximal segments to stabilize the upper extremity, while the trunk moves freely, and the center of mass is transferred between arms, to single arm stabilization, alternately. Athletes’ ability to transfer forces and shift the center of mass over the base of support could perhaps provide information to determine if an athlete is at risk of injury.20 Furthermore, the test has been presented to be easy to understand and to implement, be cost-efficient, and take up minimal space in the clinic or in the training facility.19,20
The original test protocol was developed for male athletes, who were placed in a push-up position with their toes on the ground and their hands 91.4 cm (36 inches) apart. Previous studies on the CKCUEST have investigated reliability and validity18,19,21–23 in persons with and without shoulder impingement syndrome, and indicate that the CKCUEST scores differ between players with previous injury/pain history compared with healthy players.20,24–26 Tucci et al.24 determined that the CKCUEST was reliable for both healthy adults and individuals with shoulder impingement syndrome. One preliminary study investigated differences between healthy and previously injured/in-pain baseball pitchers from high school and college.27 Sex differences in height, weight, and arm length have also been discussed in several studies, and modified CKCUEST variations of arm position and knee position have been validated.15,28–32
In previous studies, mostly baseball athletes have been investigated. To the best of the authors’ knowledge, no studies have investigated the CKCUEST performance in elite team handball players, including those playing with or without shoulder pain or a history of shoulder pain. Since many elite handball players with shoulder pain still compete on the highest national and international levels, the question therefore arises whether the level of perceived shoulder pain causes less dynamic shoulder instability within this group of athletes, and whether current and previous pain affects performance in the CKCUEST. Therefore, the purpose of this study was to investigate if the CKCUEST is an appropriate test to implement within team elite handball players to evaluate dynamic shoulder stability across sexes and in the screening of shoulder pain. The first aim was to investigate if performance on the CKCUEST and the modified CKCUEST varies among elite handball players playing with shoulder pain, previous pain, or no pain. The second aim was to investigate if the performance varies between male and female elite handball players and to evaluate if height may influence performance, as the distance between the lines is constant (91.4 cm) and thereby not compensating for height. The hypothesis was that male athletes would achieve a higher number of touches compared to female athletes, and that athletes playing with shoulder pain would have lower scores compared with the two other groups due to less dynamic shoulder stability.
MATERIALS AND METHODS
Participants
Elite team handball players were recruited from clubs in the top two divisions in Denmark and Norway, together with the top division in Romania and the Netherlands. The total group was divided into three groups: playing handball with shoulder pain, playing with previous shoulder pain, and healthy subjects and all completed a version of the CKCUEST. All players volunteered for the project after providing written and oral consent. Ethical approval was obtained from the Norwegian ethics committee REK Midt in September 2019 (ref. 7189).
All 106 players replied to a medical questionnaire regarding pain, pain history, injury history, training, and match exposure. The medical questionnaire was used to divide the players into three groups: 1) playing with shoulder pain, 2) playing with previous shoulder pain, and 3) healthy subjects. Participants included in the pain group played with shoulder pain that had been present for a minimum of four weeks and developed over time.33 The participants included with previous shoulder pain had to report no current pain and when they last registered shoulder pain (start and stop of previous shoulder pain). The participants in the healthy group never had experienced shoulder pain. Included players were required to take part in both offensive and defensive parts of the game during training and match. Players were excluded if they were recovering from musculoskeletal injuries, had been excluded from participation in the prior six weeks, or presented with pain/previous shoulder pain which was associated with a traumatic event or surgery. The presence of pain was established by the validated Oslo Sports Trauma Research Center questionnaire.33 An oral interview performed by a physical therapist was carried out to determine whether the pain registered in the group with pain and previous pain had a non-traumatic occurrence.
Test procedure
First, the player was given an oral introduction. The subject started in a push-up position, with the hands placed outside each line (3.8 cm of tape) distanced 91.4 cm (36 inches) between the lines with the feet at shoulder width. During the CKCUEST, subjects reached with alternating hands across their body to touch the athletic tape by the opposing hand as many times as possible within 15 seconds (Figure 1). The test started when the tester said “go” and ended when the tester said “stop.” To ensure correct timing, an app with a predefined time setting at 4 x 15/45 seconds was placed in front of the player. The test was performed four times with a 45-second pause in between: one submaximal test and three maximal tests. The first submaximal performance was used as a test run for the participant, with the purpose of introducing the test. The final three test performances were used in the analysis.
All elite team handball players were selected to participate in the CKCUEST, but 15 female players were not able to perform the original CKCUEST due to the wide distance between the hands compared with body anthropometrics, so they were allowed to perform the modified CKCUEST (Figure 1).19,34 The modified CKCUEST was completed with the subject starting in a push-up position on their knees and the hands placed outside the tapeline with a distance of 91.4 cm.32,34–36

The CKCUEST raw score was calculated as an average of the touches performed during the final three maximal tests.25 The test was administered by the same experienced tester, who had 10 years of experience in physical therapy and physical testing in team handball.
Data analysis
The average score of the final three maximal tests was calculated as recommended by Goldbeck and Davies.19,24 The CKCUEST has been provided with three different calculation scores to compensate for differences in body composition: 1) the raw touch score represents the number of touches the subject can perform within 15 seconds; 2) the touch score represents the number of touches performed divided by the height of the subject; and 3) the power score represents the number of touches multiplying 68% of the subject’s body weight in kilograms divided by 15 (power = 68% body mass [kg] x average number of touches / 15). The 68% corresponds to the combined body mass of the subject’s arms, head, and trunk.24
Statistical analysis
Statistical analyses were performed in SPSS version 27.0 (IBM Corp., Armonk, New York, USA). All data distributions were tested for normality with the Shapiro–Wilk test, histogram, and qq plots. Means and standard deviations (SDs) were calculated for all data, and p-values of ≤ 0.05 were considered statistically significant. A sample size calculation was based on previously published estimations containing people with and without pain in the upper limbs.20,26,27 The target participants were 88 subjects, based on an alpha of 0.05 and a power of 0.80.
All descriptive statistics and distributions of status of shoulder pain are presented with mean and SD. Correlations between the subjects’ height and the three CKCUEST scores (raw, touch, and power score) were made using Pearson’s correlation test. The interpretation of the Pearson’s correlation coefficient was made as recommended by Portney.37 A coefficient ≤0.25 was considered trivial, 0.25–0.50 low to fair, 0.50–0.75 moderate to good, and ≥ 0.75 a strong relationship. A one-way ANOVA was used to identify any statistical differences between the female participants performing the CKCUEST and the modified CKCUEST.
A two-way ANOVA was performed to identify statistical differences in the CKCUEST scores between players with shoulder pain, those with previous pain, and healthy subjects and the whole group, and between men and women. An effect size calculation was used to determine the magnitude of the effect. Effect size was evaluated with η2 (partial eta square), where 0.01<η2<0.06 constitutes a small effect, 0.06<η2<0.14 a moderate effect, and η2>0.14 a large effect.38
RESULTS
A total of 106 elite team handball players, 49 females (174 ± 3 cm, 70.4 ± 6.7 kg, and 22±4.9 years) and 57 males (190±7.5 cm, 91.6±11.4 kg, and 22 ± 5.4 years), participated in this cross-sectional study of the CKCUEST. All 106 included elite handball players were able to complete the tests: 23 playing with shoulder pain, 34 with previous pain, and 49 with no pain. A total of 91 players performed the CKCUEST, 34 females (175 ± 5 cm, 72 ± 6.8 kg, and 22.7±4 years) and 57 males, and a total of 15 female players (172 ± 6 cm, 66.8 ± 4.6 kg, and 20.3±6 years) performed the modified CKCUEST.
Performance among players with pain, previous pain, and no pain
Across sexes, no significant differences between pain groups were found in any of the CKCUEST scores: raw score (F=0.651, p=0.52, η2 =0.02), touch score (F=1.23, p=0.30, η2=0.03), and power score (F=0.71, p=0.50, η2=0.02), all with small effect sizes. No significant differences were found within the female group: raw score (F=0.913, p=0.41, η2=0.06), touch score (F=1.20, p=0.31, η2=0.07), and power score (F=0.41, p=0.67, η2=0.03). Also, no significant differences were found within the male group: raw score (F=0.835, p=0.44, η2=0.03), touch score (F=1.47 p=0.24, η2 = 0.05), and power score (F=2.18, p=0.12, η2=0.08). (Table 1).
Performance between men and women
Significant differences and large effect sizes were found between the female and male team handball players when comparing all three CKCUEST scores (p<0.01): raw score (F=125, p<0.01, η2=0.59), touch score (F=107, p<0.01, η2=0.71), and power score (F=82.6, p <0.01, η2=0.48) (Table 2).
Performance in the modified and original CKCUEST
The female athletes performing the modified test had an average height of 1.72.±0.06 m compared to 1.75±0.05 m for the females in the regular test, but no significant differences were found in any of the CKCUEST scores between the females performing the CKCUEST and the modified test in any of the scores: raw score (F=1.39, p=0.244, η2=0.03), touch score (F=2.55, p=0.12, η2=0.05), and power score (F=0.09, p=0.76, η2<0.01), all with small effect sizes. Furthermore, no significant difference was found in the CKCUEST scores in the three groups: pain, previous pain, and healthy players performing the modified CKCUEST (Table 3).
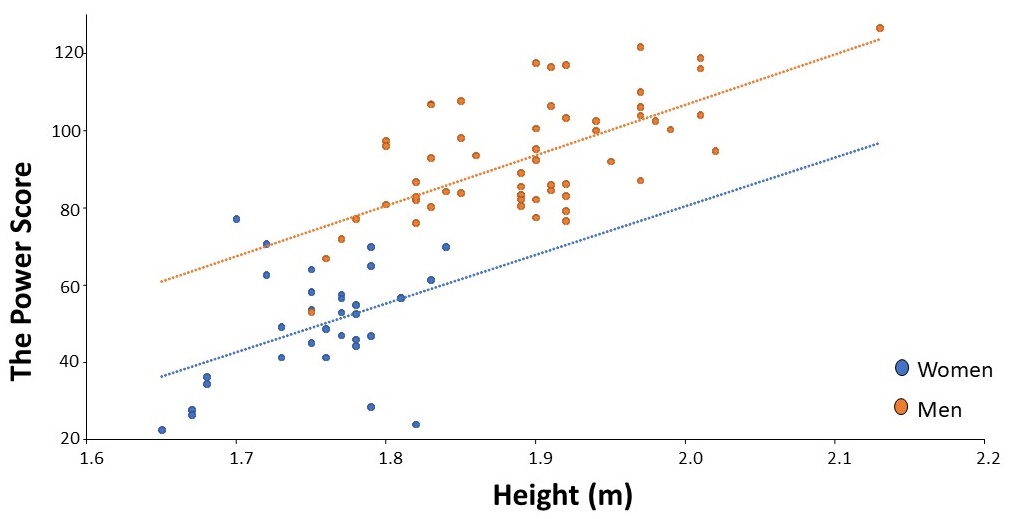
Correlation between performance and height
Significant correlations were found in both the male and female groups between height and the power score. Males had a significant moderately positive correlation (r=0.661, p≤0.001) compared to the female athletes, who presented a significant fair correlation (r=0.434, p=0.01). A fair, non-significant correlation (r=0.332, p=0.06) was found in the female group between the raw score and height. In the modified CKCUEST, a significant moderate correlation was found between height and power score (r=0.55, p=0.03), while no significant correlations were found with the raw (r=0.49, p=0.07) and touch scores (r=0.40, p=0.14) (Figure 2).

DISCUSSION
The purpose of this study was to investigate whether the CKCUEST and the modified CKCUEST are appropriate clinical assessment tools for dynamic shoulder stability in male and female elite handball players. Furthermore, the study sought to evaluate if variation is detectable in the performance of the CKCUEST between players performing with shoulder pain, previous pain, and no pain, and if performance varies across gender and height. The main findings were that significant differences were found in the raw and touch CKCUEST scores between male and female participants, but not among the players playing with shoulder pain, previous pain, and no pain. A significant correlation between height and the power score was found in both groups.
In the current study, the male athletes achieved a significantly higher score compared to the female elite athletes. A higher number of touches indicates the athlete found it easier to stabilize and move the center of mass from one arm to another, which demands high-power neuromuscular activity, motor control, and proprioception. The current findings are consistent with the study by Borms and Cools17 in which the male players had a higher number of touches compared to female players. However, Borms and Cools17 presented a higher number of touches than in the present study in both men (27.4±2.7) and women (20.8±2.7). Additionally, higher scores were found in college baseball in the studies by Taylor et al.39 at 25±4.5 and Roush et al.40 at 30.4±3.9, while Schilling and Elazzazi34 presented scores from college baseball, where the pitchers scored 19.1±4.5 and the other positions scored 18.8±3.5.
Prior studies have performed the CKCUEST with small differences in the test setting. Cogley et al.41 showed that a different hand placement during a push-up alters upper-body muscle activity and therefore changes the muscle work. Furthermore, Schilling and Elazzazi34 performed the test with a distance of 36 inches, where the middle of the hands was placed on top of the two pieces of tape, not outside the tape. Negrete et al.42 had the push-up position with the hands within the two pieces of tape, and Taylor et al.39 started with the arms in a push-up under the shoulders. The combination of small differences in test setting and different population groups may influence the variety in number of touches observed; therefore, making a comparison of the performance across sexes and sports can be difficult.
This study observed higher numbers of touches performed by the male athletes compared with the female elite handball players. The differences in performance may be explained by the anthropometric differences measured between the male and female subjects. Powell et al.16 found that the length of the arm has a significant positive effect on the CKCUEST score. Unfortunately, Powell et al. did not measure the length of the participants’ arms but found a fair to moderate significant correlation between height and sex within the elite team handball players. Taking an anthropometric perspective, a person with longer arms has a shorter distance of transfer in the body and an advantage in performing the CKCUEST. Furthermore, Callaway et al.28 argued that the distance of 91.44 cm has not been justified, and they therefore investigated the CKCUEST with modified test settings in healthy male subjects and compared them to the original CKCUEST. They recommended clinicians to use a width matching 50% of the individual’s height, which showed excellent repeated measures reliability and the smallest minimal detectable change. This recommendation was used in the present study with the modified CKCUEST. The female athletes were instructed to perform the CKCUEST but could choose to perform the modified test if they were unable to perform the original CKCUEST (Figure 1). In general, the shorter female athletes (1.72±0.06 m vs. 1.75±0.05 m) chose the modified CKCUEST, with similar results between the two groups, indicating that perhaps the CKUEST needs to be modified for arm length or height, due to the unfavorably long hand-to-hand distance.16 Based on these findings, it cannot be recommended to use scores from the original CKCUEST to evaluate performance across sexes in team elite handball players, even though the touch and power scores try to compensate for differences in weight and height within and across genders. However, more studies are needed to confirm these findings.
The current study did not find any significant differences in performance within the three groups measured by the numbers of touches performed. Previous literature19,43 has presented the CKUEST as an option to evaluate the dynamic stability of the shoulder and upper body by moving the center of mass from side to side. It was expected by the authors that this dynamic shoulder and upper body stability would be affected by shoulder pain. The painful shoulder would cause more time spent on the injured side together with other compensating movement patterns, as shown by Barfield et al.27 They showed that high school and collegiate baseball pitchers who were previously injured had less pelvic rotation and dominant hip abduction during the touch of the non-dominant hand compared to the healthy group. This indicates kinematic changes that could affect the CKUEST scores between the groups. The fact that no differences were found between the groups can be explained by several possibilities. Firstly, it is not known if decreased dynamic stability is the cause of shoulder pain in the pain and previous-pain groups. Forty-four to 75% of senior players have experienced shoulder pain, and 12–40% are playing with modifications, but studies have not presented the distribution of diagnosed reasons for pain. This group of elite athletes presented with a high level of physical fitness but may have experienced challenges when performing a bilateral closed kinetic exercise when their specialized movement pattern is a unilateral open kinetic chain. Furthermore, the included athletes were all still active participants in handball. If the shoulder pain kept them from playing, a difference in score may have been observed, as Tucci et al.24 observed in players with shoulder impingement syndrome who scored only 10–12 touches.
The question of whether the CKCUEST can be used as a screening tool in elite handball players playing with pain, previous pain, or no pain can be answered in the negative. However, the CKCUEST might be used to identify the risk for in-season shoulder injury, as has been suggested by Pontillo et al.20 In a prospective study on American college football players, they found a trend in the athletes developing a shoulder injury during the season. The authors suggested that a score of fewer than 21 touches in male athletes would indicate a higher risk of developing a shoulder injury. However, they used a small cohort design including 26 male athletes; they did not report whether the injury stopped the American football athletes from participating completely; and the CKCUEST was included as a functional test but was only performed two times with a one-minute break, in contrast to the recommendations of Goldbeck and Davies.19 When comparing their recommendation to the findings of the current study, all included elite handball players performed more than 21 raw touches (Table 1). Therefore, the suggestion of 21 raw touches is perhaps a little conservative for the group of team elite handball athletes investigated in this study.
The CKCUEST did not show any statistically significant differences between the players playing with shoulder pain, previous pain, and no pain, which raises the question of the relevance of the test as part of a test battery or screening tool to detect shoulder pain among handball players who are still playing. The cause of shoulder pain among overhead athletes is often a combination of several risk factors. To prevent shoulder injuries in pre- and in-season athletes, the use of a test battery of strength, fatigue, and functional testing may be helpful in identifying who is at higher risk for sustaining a shoulder injury.6,7,44 But few non-professional handball clubs have the possibility to create such a medical setting; therefore, it is important to continue using easily implemented clinical tools that could help in screening risks for shoulder injuries.
LIMITATIONS
A growing number of performance assessments are available for clinicians to use to screen and evaluate throwing athletes. The CKCUEST has been presented with moderate to strong reliability.18,45,46 But the interpretation of the current results must still be viewed within the limitations of the study. Only a small sample performed the modified CKUEST test, and an uneven group size in the number of participants with previous or current shoulder pain compared to healthy subjects must be considered. Finally, this study has reported performance in the CKCUEST with a cross-sectional design, and it has not been assessed whether the CKCUEST can be a relevant test regarding use for injury prevention and return to performance decision-making. Future studies should include the CKCUEST in longitudinal study designs and investigate the ability to predict shoulder pain and the readiness to return to activities, resume competition, or continue further rehabilitation in elite team handball players.
CONCLUSION
The results of the current study provide novel data on CKCUEST performance in team elite handball players playing with shoulder pain, previous shoulder pain, and no shoulder pain. A significant difference between male and female athletes indicates that a comparison in performance across sexes is not suitable, due to the possible positive influence of height in the test setup. But within the female group, performances of the CKCUEST and the modified CKCUEST were comparable. Additionally, the CKCUEST was not able to differentiate among elite handball players who are still playing with shoulder pain, previous shoulder pain, and no pain.
ACKNOWLEDGEMENTS
Many have contributed to this project. The authors would particularly like to thank the medical staff in the clubs and Olympic Centers and all the elite handball players for supporting and participating in the project.
CONFLICT OF INTEREST
The authors have no conflict of interest to declare.