INTRODUCTION
Despite continued improvements in the understanding of the overhead throwing motion, injuries to the upper extremities of baseball pitchers continue to rise across all levels of play.1–4 Efforts to return pitchers to their pre-injury level of performance remains a critical, yet challenging task for sports medicine physicians, physical therapists, athletic trainers, and other rehabilitation specialists. Successful rehabilitation of baseball pitchers relies on a gradual building of strength, flexibility, and endurance to meet the demands of competition. With or without surgical intervention, an interval throwing program (ITP) remains the cornerstone by which throwing athletes systematically return.5 Once a pitcher is cleared by medical staff, he may then pursue his competitive training (long-toss, weighted balls, bullpen sessions, etc.) and pitching in games.
Traditional ITPs have relied on a generic, standardized prescription of throwing activities that change in volume, distance, and effort exerted over a fixed timeframe.6 The distance, volume, and intensity of throws are progressively overloaded to gradually expose the pitcher to mechanical stress, resulting in tissue adaptation to the increased demands of throwing.7 In general, an ITP is comprised of a flat-ground (sometimes referred to as long-toss) progression with increasing distances starting somewhere from 30 ft to 60 ft out to 120 ft. After completing the flat-ground progression asymptomatically, the pitcher transitions to pitching from the mound at regulation distances (60.5 ft) with graduated intensities, often starting at 50% effort. Some ITPs have prescribed pitchers to throw off the mound at reduced distances of 45 ft before transitioning to the full 60.5 ft.
Recent advancements in the assessment of throwing biomechanics have scrutinized how factors such as throwing distance and ball velocity impact stresses experienced at the shoulder and elbow.8,9 Biomechanical metrics, such as elbow varus torque, offer objective and potentially more accurate data about training loads in which pitchers experience. For example, Melugin et al10 demonstrated that a reduction in perceived effort did not correlate with the same percent reduction in ball velocity and elbow varus torque causing variability in predicted workloads. Metrics, such as the acute:chronic workload ratio (ACWR), employ biomechanical parameters to evaluate whether training loads experienced by a rehabilitating athlete occur in a graduated manner.11,12 Previous research investigating ACWR has reported increased injury risk occurs when the workload ratio either exceeds 1.3 or drops below 0.7.13–16 Together, biomechanical data and objective metrics for training loads afford an opportunity to optimize ITPs to avoid excessive variations in training loads and, potentially, avoid setbacks and recurrent injury during rehabilitation.
The purpose of this study was to evaluate three prominent ITPs frequently utilized among rehabilitating baseball pitchers and assess whether contemporary ITPs produce training loads that increase in a controlled, graduated manner. It was hypothesized that ITPs commonly employed by baseball pitchers would have excessive variation in training workloads that sometimes produce ACWR outside the safe range of 0.7 - 1.3. Therefore, a secondary aim of the study was to devise an ITP that produced training loads which increased steadily over time, thereby reducing the potential risk of re-injury during rehabilitation and more efficiently condition a pitcher for return to competition.
METHODS
Interval Throwing Programs (ITPs)
Interval throwing program protocols were identified at three sports medicine institutions affiliated with Major League Baseball. Individual ITPs were selected based on their public and academic prominence pertaining to the treatment of professional baseball pitchers.17,18 The selected ITPs are among the most utilized in the rehabilitation process for return to throw for pitchers. The three throwing programs were from the American Sports Medicine Institute (Program A, Supplement 1), the Kerlan-Jobe Institute (Program B, Supplement 2), and Hospital for Special Surgery (Program C, Supplement 3), respectively.
Calculation of Elbow Varus Torque and Workload
In order to determine elbow varus torque with each throw, data were mined from Motus Global’s MotusBaseball sensor (now Driveline Pulse; Driveline Baseball, Kent, WA) database. Previous research has shown that the Motus sensor’s measures correlate well with 3D motion capture laboratory measures19,20 and provides precise and reproducible data.10,21 A total of 238,611 anonymized flat-ground throws were extracted from one NCAA-Division 1 level team over the course of two years. These throws were taken by healthy college pitchers (n=34, 186.02 ± 7.3 cm, 89.4 ± 10.8 kg). Of these, 111,196 flat-ground throws were tagged by distance, ranging from 30 ft and 300 ft. Distance categories with over 1,000 throws per distance were used in the model. A 2nd order polynomial regression created a relationship between throwing distance (x in ft) and peak elbow varus torque (Nm) (Equation 1).
τvalgus=−0.000579x2+0.194x+36.230;r2=0.986
The workload of each throw (WLThrow) was computed by exponentially weighting the elbow varus torque value to 1.3 (Equation 2). This exponential weight was chosen based on NASA’s ‘Daily Load Stimulus’ research regarding mechanical load and gravity.22
WLThrow=τvalgus1.3
Daily workloads (WLDay) were computed as the total sum of workload of each throw (Equation 3).
WLDay= Throw=n∑Throw=1WLThrow
Acute workloads (WLAcute) were computed as a rolling 7-day average of daily workload (Equation 4).13
WLAcute=17day=7∑day=1WLday
Chronic workloads (WLChronic) were computed as a rolling 28-day average of daily workload (Equation 5).13
WLChronic=128Day=28∑Day=1WLDay
Finally, the ACWR was computed as the acute workload divided by the chronic workload (Equation 6).
ACWR=WLAcuteWLChronic
Workloads (i.e. daily, acute, chronic, and ACWR) were built from the prescribed throwing for each program. Previous research investigating ACWR has reported increased injury risk occurs when the workload ratio either exceeds 1.3 or drops below 0.7.13–15 Therefore, the ACWR ‘safe’ range was coded as anything between 0.8-1.3.
Each ITP consisted of various sequential phases; a pitcher must complete each phase pain-free before progressing to the next phase. In Program A, pitchers were instructed to throw every other day and perform each phase two times before advancing to the next phase. Program B instructed pitchers to throw three to four times per week. To account for this, one week was coded throwing three times and the next week was throwing four times; this alternated between the two for the whole program. Additionally, phases in Program B were separated by month without specifying how many times each phase should be repeated, therefore it was assumed four weeks of throwing for each month. Program C instructed players to throw every three days and to complete each phase three times before progressing to the next one.
While an ideal ITP would explicitly state which days to throw, the number of throws per day, and clearly defined distances, this exact information was not available in each of the three programs. Program C was the only program to explicitly state the number of throws to perform at each phase with specific distances. Program A provided a range of throws starting at 75 ft and varied 5-15 throws at each phase after. Program B had a range of throws for each phase and varied 5-20 throws and a range of throwing distance (i.e. 40-45 ft, 60-70 ft). To standardize the number of throws for each phase in the programs that did not have an exact number, the median of the provided range was used. For example, if the program stated to throw 20-25 times at a given distance, the throws coded were 23. In order to standardize Program B that used distance ranges, the distance closest to the 15 ft increments used in the two other programs was used (i.e. 40-45 ft, 45 ft distance was used).
For all ITPs, throws in the flat-ground progression were instructed to be thrown as ‘catch’ and not meant as maximal effort throwing. These flat-ground throws were not to be thrown with a pitching motion and all were programmed using the flat-ground polynomial regression torques. All programs allowed crow-hop/shuffle at longer distances (starting at 75 ft), which was accounted for in the polynomial regression. Program C did not prescribe warm-up throws. Program A stated warm-up throws should start at 30-45 ft and then progress to the starting distance for the phase, but the quantity of throws was not provided for these ‘warm-ups’. Program B prescribed 10 throws at 40 ft as a ‘warm-up’ and ‘cool down’. In order to standardize across Program A and C, it was assumed ‘warm-up’ throws to be 5 throws at each distance – increasing by 15 ft until reaching the starting throwing distance for that day. Additionally, if a program stated throws could be taken if the athlete desired, then 5 throws at that distance (similar to warm-up throws) were coded. Program C provided an optional three weeks of flat-ground (phases 13-16), this was not coded as they were considered optional.
All three programs delineated throwing intensity during the mound phase (e.g., 20 throws at 75%). Asking pitchers to throw with graded effort is a difficult and sometimes inaccurate task. Previous research has shown that there was not a proportionate decrease in ball velocity or elbow varus torque to perceived effort when pitching off the mound.23,24 Melugin et al10 reported that when pitchers were asked to throw 50% effort, elbow varus torque was 86% of maximum torque and when throwing 75% effort, elbow varus torque was 93% of maximum torque. In order to codify for mound intensity, the average 100% effort torque from Melguin et al’s study 74 Nm) was used and a linear regression model was built using the three efforts and resulting torques (Equation 7). This allowed for the differentiation of prescribed intensity and to build the resulting torque for each program.
τactual=τmaximum(0.28∗(perceived intensity)+72)100
Lastly, two programs (Program A and B) prescribed off-speed pitches when the pitcher was close to resuming game throwing, whereas Program C did not specifically differentiate between pitch types. Previous research has shown that resultant loads in the throwing arm are similar for the fastball and curveball in pitchers.25–27 Thus, pitch types were not differentiated and fastball elbow varus torque was used for the workload calculations.
Model ITP for Optimizing Work Load Progression
Using the results of the three ITPs, a novel computationally-optimized workload ITP model was created (Supplement 4). This model was developed to maintain an optimal ACWR, while also steadily increasing the chronic workload throughout the throwing program. The novel model utilized non-linear throw count increments, while steadily increasing throw counts and distances with variability in the daily amounts. In current programs, cyclic loading and consistent off-days in the protocols (i.e. throwing every other day) led to detrimental ACWR. To address this, variable off days were implemented with throwers not throwing on consecutive days over what would be considered a “weekend” until week 16 where a light throwing day was implemented. Throwing volume was gradually built up along with increased throw distance, until 120 ft throwing distance was reached; then the protocol transitioned into throwing from the mound. The mound progression was gradually built up with pitch counts to reach an optimal chronic workload of 13.8.13 The last week of the program’s mound days were delineated as live pitching sessions where players were allowed to pitch to a hitter but still have constrained pitch counts.
RESULTS
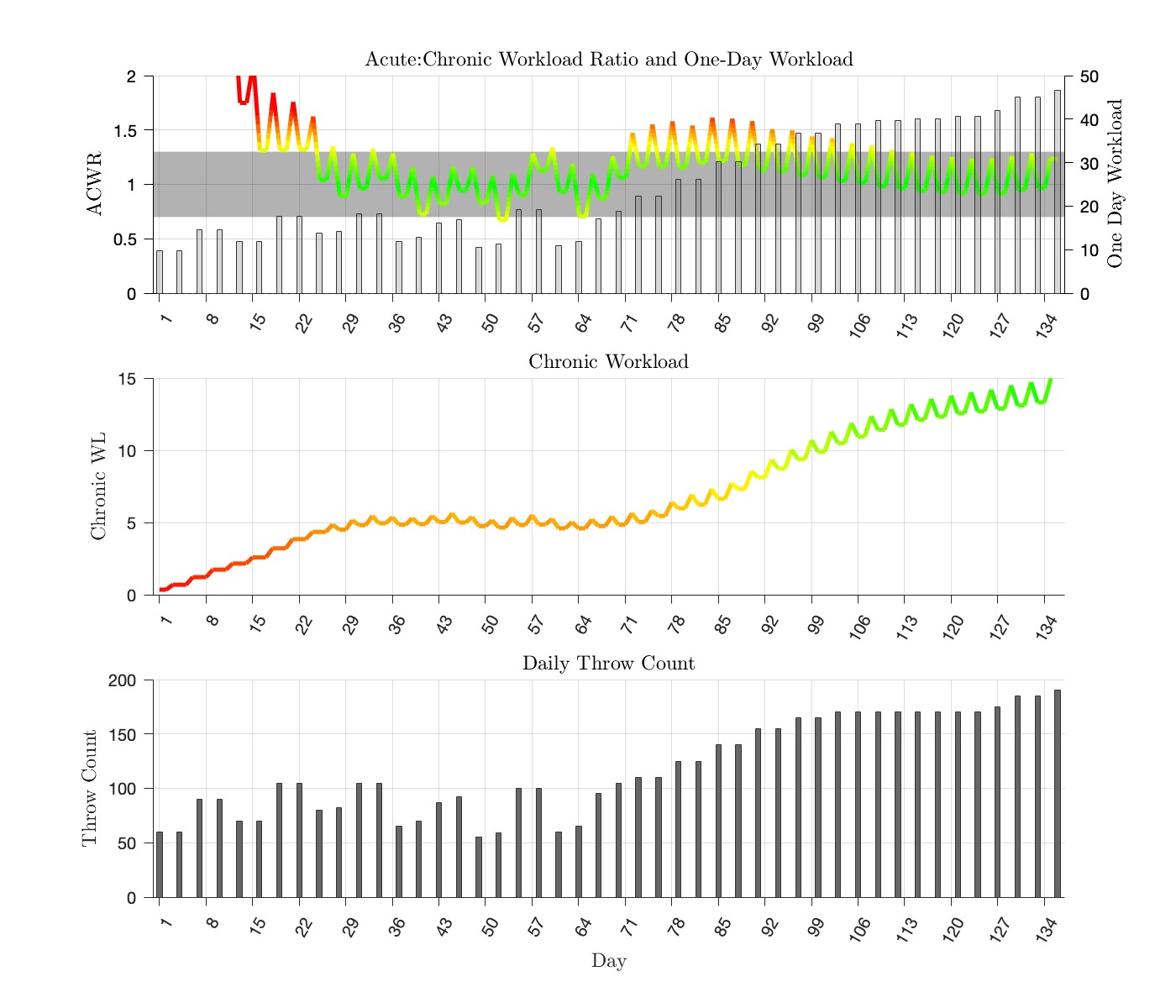
Each ITP exhibited a unique progression of throwing distances, quantities, and days to create different workload profiles. The chronic workload in the denominator of ACWR increases during the first 28 days, causing all four programs to have large spikes in ACWR early in this initial period.
Program A consisted of a 136-day schedule. The first 72 days were the flat-ground phase and included 24 days of throwing (Figure 1). The final 64 days were the mound phase and included 22 days of throwing. The program finished with a chronic workload of 15.0. During the program, there were 19 times the ACWR spiked above or below the safe range.

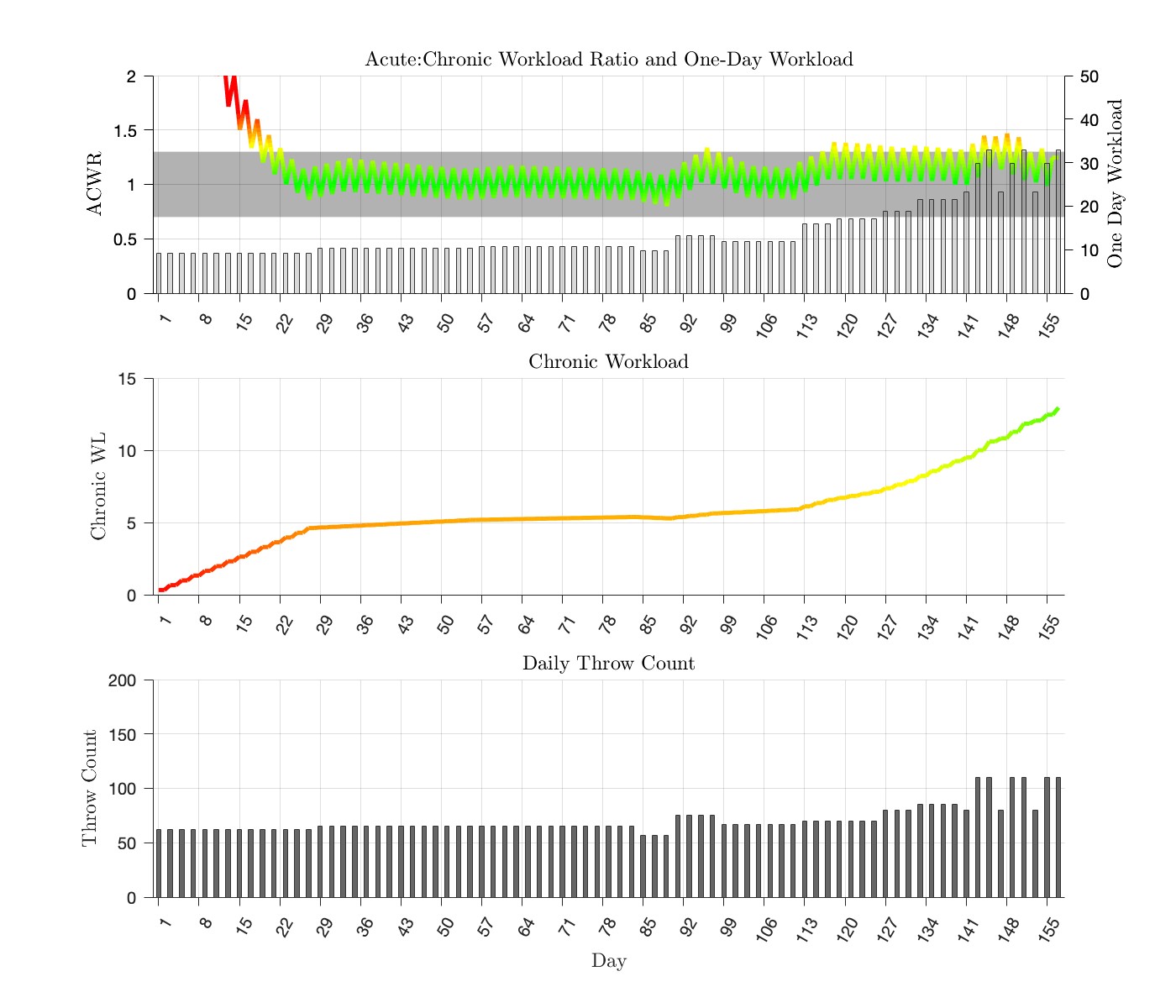
Program B consisted of a 157-day schedule (Figure 2). A total of 56 out of 111 days were spent throwing in the flat-ground progression. The mound progression consisted of 23 throwing days out of 46 total days. The program finished with a chronic workload of 13.0. During the program there were 21 times the ACWR spiked above or below the ‘safe’ range.

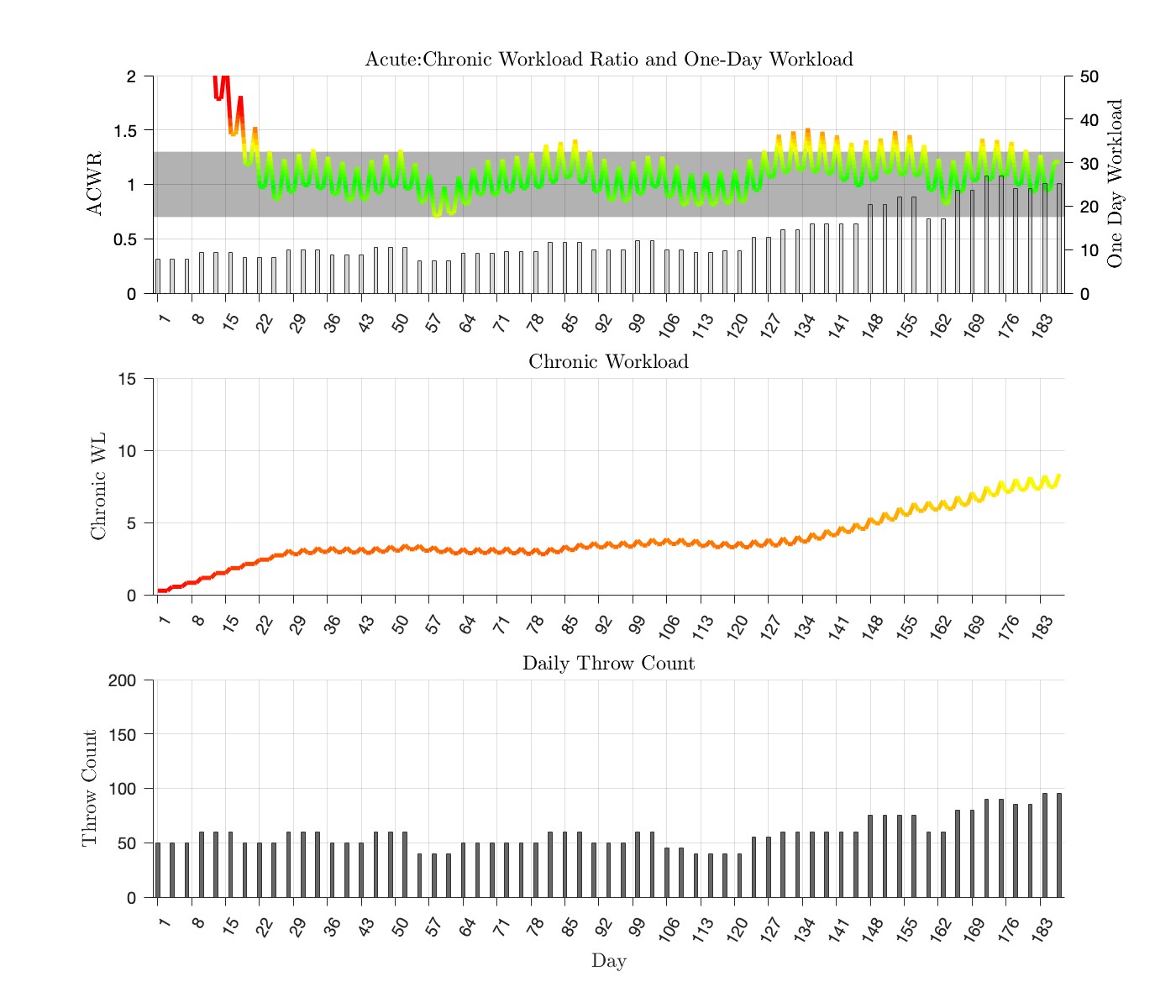
Program C consisted of a 187-day schedule (Figure 3). There were 36 throwing days in the 106 days of the flat-ground progression. The mound progression consisted of 28 throwing days out of 81 total days. The program finished with a chronic workload of 8.4. During the program there were 23 times the ACWR spiked above or fell below the ‘safe’ range.

Novel Interval Throwing Program to Optimize Workload Progression
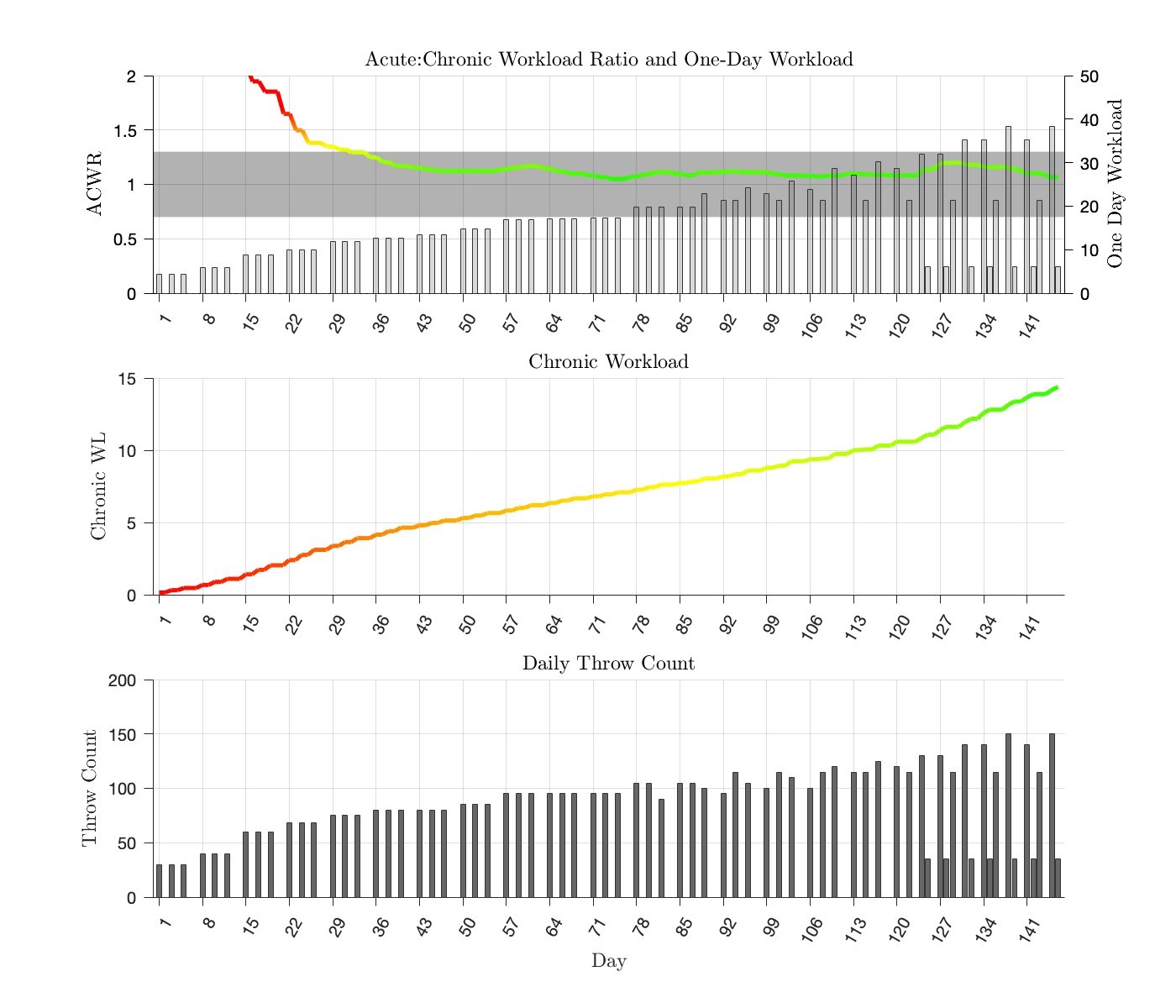
The newly modeled optimized ITP consisted of a 146-day schedule (Figure 4). The features of the optimized ITP were reverse-engineered using computational modeling to derive a graduated increase in ACWR. There were 33 days of throwing within the 77 days of the flat-ground progression. The mound progression consisted of 37 throwing days out of 70 total days. The program finished with a chronic workload of 14.2. The program was built so there were no spikes in ACWR once 28 days of throwing was accomplished.

DISCUSSION
There are a plethora of ITPs circulating in the baseball community, as orthopedic surgeons often utilize unique ITPs for their recovering pitchers. ITPs have traditionally not been based on relevant physiologic metrics like workload (acute, chronic, and ACWR) and instead on anecdotal, clinician-directed experiences. The principal finding from this study is that several prominent, contemporary ITPs utilized by injured baseball pitchers confer inconsistent progression of throwing workloads.
A recent study emphasized the dramatic variability in rehabilitation and throwing programs after ulnar collateral ligament reconstruction (UCLr) surgery.28 Each program varied in its instructions, number of days to complete the program, distance, volume, intensity, mechanics, and pitch type. In a more recent study, Griffith et al29 reported significant variability between 717 professional pitchers undergoing rehabilitation after UCLr and the timing of throwing progressions varied widely. Accounting for individual variability, pain, recovery, and adherence to the exact program is virtually impossible for all programs. The variability found in these studies, as well as in the present analysis, highlights the potential for optimizing rehabilitation programs based on objective metrics. In turn, a newly devised ITP modeled to reduce the variability in workload may reduce the risk of set-back or recurrent injury by providing a steady incremental increase of tissue loading during throwing rehabilitation.
This study’s findings rely upon ACWR as a surrogate marker for evaluating how ITPs progress baseball pitchers in their rehabilitation. Increased ACWR has been linked to increased risk of suffering a time loss injury across a variety of sports.11 Moreover, Gabbett et al30 demonstrated that the correlation between higher ACWR and injury risk was consistent across multiple methods of calculating ACWR. The present study’s application of ACWR builds upon prior work assessing performance progression in other sports10 including soccer,14 rugby,31 gymnastics,32 and cricket,33 all of which advocate for maintaining consistent ACWR ranges. When building the ACWR, this study used the assumption that at the beginning of the ITP, no throws had been completed for the previous 28 days. However, because of large variations in rehabilitation protocols for UCLr before throwing a baseball even takes place, this assumption may or may not be correct. There has been a recent emphasis for pitchers to perform plyometric training in rehabilitation which can result in added elbow varus torque to the throwing arm before starting their ITP.34 If plyometric training is being performed during rehabilitation, then it is possible that throwers are not starting at 0 for workload on Day 1 of the ITP and the ACWR would be altered at the beginning stages of throwing. However, the only true way for the throwing arm to experience the same forces and torques during the throwing motion is to actually throw a ball; therefore, this assumption is reasonable. It is hard to know if this ‘skyrocket’ in ACWR during the first 28 days of throwing is useful or accurate; but caution should be taken during the first month of throwing.
Within baseball, higher ACWR has been associated with increased injury risk among varsity high school pitchers.13 In a cohort of 18 high school pitchers, whose throws were tracked for six months using a wearable MotusTHROW™ sensor, five out of six throwing-related injuries occurred in pitchers whose ACWR exceed 1.27.13 Pitchers whose workload exceeded this threshold value exhibited an injury risk nearly 15-times that of those below this value. In our study, a pitcher who simulated Programs A, B, and C exceeded this ACWR threshold 18-23 times starting from Day 28; while our optimized program was created to not deviate from the safe ACWR range of 0.7-1.3. Extrapolation from prior data of ACWR threshold values on varying levels of baseball pitchers is needed and further study is necessary to delineate optimal ACWR values in baseball pitchers. Nonetheless, the present data align with the available literature suggesting that existing ITPs are not optimized to load the throwing arm of a rehabilitating pitcher.
Gradual building of the chronic workload throughout an ITP is vital to help mitigate spikes in ACWR when there are high acute workload days. In this way, high chronic workloads are thought to be protective. In middle-school aged athletes, it was reported that high chronic workloads were associated with reduced risk of injury.35 This protective effect of chronic workload has also been reported in both rugby and cricket.31,33 However, limited studies in baseball link workload based off each throw and injury. In high school players, Mehta et al36 reported players with higher chronic workloads were associated with increased risk of injury compared to players with lower chronic workloads. In-season chronic workloads have been reported in high school pitchers to be between 12-15.36 This is similar in college and professional pitchers, as reported by Motus Global (unpublished). Programs A and B had chronic workloads when the programs finished between 13-15; similar to the Optimized program (Program D) that was built. Program C finished well below the targeted average at 8, even though this program also had the greatest duration of days (187).
Appropriate timing in the implementation of an ITP is crucial to ensure the safe return of a throwing athlete to competition. For example, the minimum duration of time and rehabilitation required before an athlete can safely return to throwing after UCLr has not been determined.37 Many factors can influence the ideal time course for initiating an ITP, such as time from surgery, level of competition, time of season, surgeon’s preference, and successful progression through physical therapy. In a recent review, Griffith et al38 included 14 studies tracking return to sport (RTS) after UCLr and reported time from surgery was the most common RTS criterion used and was reported in 100% of the studies. However, there was no consensus on how much time was adequate for rehabilitation before returning, with time frames ranging from 4-16 months.38 Conversely, in a separate systematic review the most common return to play criterion was completion of an ITP (87%; 13 out of 15 studies) and found players started the ITP on average 16.7 weeks after surgery (range 12-18 weeks).39 The optimal wait period following injury or surgery to initiate an ITP is likely highly individualized. We believe objective testing is vital to proper progression into starting a throwing program. In a recent study, 25% of competitive pitchers did not pass an objective return to throw protocol at the time of clearance by their surgeon.40 The study also reported lack of plyometric exercises in the rehabilitation process as the most common reason for failing their return to throw protocol. Measures such as range of motion, grip strength, arm strength, and endurance should be used to properly progress a pitcher into throwing; however, further investigations can help elucidate specific attributes of injury, surgery, and/or objective benchmarks to better guide athletes on when to initiate an ITP.
Interval throwing programs use distance as a measure of intensity in lieu of prescribed efforts, radar guns, or wearable technology. While some programs explicitly state to throw with a certain amount of intensity or effort, others do not. Pitchers are frequently unable to accurately assess their throwing effort or intensity, particularly when they are rehabilitating from an injury. This becomes more of an obstacle once a player gets to the mound progression as some programs instruct players to throw with as little as 50% effort. This is not a feasible, or even an easy, task for a pitcher to do. When pitchers were asked to throw with decreased intensity, they did not decrease elbow varus torque or ball velocity at the same rate as their perceived intensity.23 Anecdotally, players do not like throwing at dramatically reduced efforts and find it difficult to get the ball to the desired target. Reduced efforts also cause deleterious changes in throwing mechanics and timing of the throw.24,41 The Optimized Protocol was created so that pitchers throw with ‘intent’ and build up their workload during the flat-ground progression, so that once they step on the mound during the second part of the program, their effort does not need to be decreased.
Concern for potentially volatile changes in tissue stress among prevailing ITPs stimulated the design of a novel ITP aimed to deliver appropriate, progressive workloads to the rehabilitating pitcher. In this model, throwing variables such as throwing frequency, throwing distance, and throwing effort were generated based upon calculated ACWR. The ITP’s design is compatible with emerging biofeedback technologies that allow for real-time monitoring of torques experienced by an individual athlete.42,43 Applying such technology can enable rehabilitation specialists to individualize these programs by modifying quantities of throws, arm speeds, distances, and the relative amount of flat-ground versus mound-based throwing to titrate actual workload. The Optimized Protocol, along with other new rehabilitation tools, require long-term evaluation to determine whether they result in meaningful reductions in injuries as well as effectively prepare the pitcher for return to sport. Nonetheless, the ITP was conceptualized as an individualized and proactive form of rehabilitation that is responsive to objective, real-time biometric data.5 Future innovations in throwing rehabilitation will likely benefit from aiming at this objective.
This study must be considered within the context of its limitations. Rehabilitation of the baseball pitcher following injury is a highly individualized process and the current analyses of both existing and proposed ITPs do not account for how such protocols are implemented and tailored to an individual pitcher. The absolute values of elbow varus torque and workloads calculated in the present analysis were determined using data reported by Melugin et al10 and therefore may vary for pitchers of different size, throwing mechanics, prior injury, etc.44,45 Nonetheless, despite increased emphasis on dynamic, interactive rehabilitation that respond to athlete biofeedback, formalized throwing programs remain a cornerstone of modern rehabilitation and merit further optimization. The provided computational model of throwing workload was predicated on biomechanical studies of elbow varus torque experienced by pitchers at varying distances, effort level, and field surface (flat-ground vs. mound) and may therefore be most applicable to pitchers recovering from elbow-related injuries.46–48 However, further study is needed to evaluate the impact of ITPs on other biomechanical variables, such as shoulder distraction forces and the addition of various pitch types. Interval throwing programs are supposed to enable a pitcher to return to proper throwing mechanics upon completion of the program; however, measuring proper kinematics of the throw are beyond the scope of this study. While the Optimized Protocol was designed to safely ramp pitchers up and maintain ACWR within a safe range, rehabilitating pitchers commonly experience one or more setbacks during the return-to-throw process, causing them to stop throwing or repeat a subset of an ITP. For all programs, the rehabilitation team must recognize and accommodate an ITP to an individual pitcher. In attempts to simulate a set-back, we changed the Optimal Program to have a week repeated once, twice, and three times and there was no change in the ACWR; however, the final chronic number was greater. Additionally, while the codified workload was specific for the throwing arm, other factors such as rate of perceived exertion from previous throwing day, recovery, sleep, nutrition, cumulative physical and mental stress, and hydration likely influence perceived effort and workload in the pitcher. Future investigation is needed to characterize and quantify such variables for implementation into a computational-based ITP. The time intervals for acute (7 days) and chronic (28 days) workloads might be inaccurate for a baseball pitcher starting on a 5-day rotation. There is also concern for the conceptual basis of ACWR and the statistical faults that arise from these calculations.49,50
CONCLUSION
Existing ITPs utilized for rehabilitation of baseball pitchers exhibit wide and inconsistent variation in the rate of throwing load progression. Computational modeling may facilitate more incremental workload progression in ITPs, thereby reducing the risk of injury during rehabilitation and more efficiently condition a pitcher for return to competition.