


INTRODUCTION
In 1997, Physical Therapists and Athletic Trainers from the International Association for Dance Medicine and Science (IADMS) called for an injury surveillance screening protocol for the dance community.1,2 Similar to the process used in athletes in competitive sports, the surveillance program would include a preseason screen of dancers’ intrinsic and extrinsic risk factors and subsequent injury occurrence reports for each dancer.2 The purpose of preseason screening was not only to uncover injuries and health issues, but also to screen for factors that may predispose the individual to injury, assess physical maturation, determine physical fitness, and educate the dancer regarding injury prevention and proper nutrition. Additionally, the screening period can serve to establish a positive relationship between young dancers and physical therapists or other healthcare professionals to promote safe, healthy participation in dance.1–5
Adolescent dancers could benefit greatly from pre and mid-season screening tools. This population - dancers between the ages of ten and nineteen6 - experience tremendous physical and psychological changes and risk of injury.7 Adolescents undergo rapid growth spurts that impact both their musculoskeletal and nervous systems.8–15 Strength and flexibility can temporarily decrease, and the young dancer can experience a period of incoordination. These changes may be experienced as a temporary decline in technique.8,10–12 This may lead dancers or dance teachers to push harder for an idealized aesthetic, instead of understanding the limitations of this temporary growth period, putting the young dancer at risk for overuse injury.11 Rates of injury in adolescent dancers range from .77 to 4.7 per thousand dance hours7,15,16 with overuse accounting for the majority of injuries.7,15
Faulty technique has also been cited as a contributor to dance injury.17–19 A growing number of clinicians are including technique assessments in wellness screens. However, there is limited research confirming the reliability of dance technique screening in adolescent dancers.18,20–22 The use of assessments that have not been validated or tested for reliability may undermine the effectiveness of conducting dancer screens. Before any measurement instruments or assessment tools can be used for research or clinical applications, their reliability should be established.23
The physical changes experienced by dancers can also lead to psychological hurdles. As their bodies change, some dancers feel as if their physique is shifting away from the ideal dancer’s body.11 This may cause dancers to consume fewer calories to maintain a “ballet” body, putting them at increased risk for developing eating disorders, relative energy deficiency in sport syndrome (RED-S), (formerly female athlete triad) and injury.4,24–26 These simultaneous physical and psychological changes make the adolescent dancer particularly susceptible to injury.9,10
In the last 20 years, there has been a substantial effort to build standardized preseason screens for professional dancers. Little has been done to produce standardized screens of the same caliber for adolescent dancers, though several screens for young dancers exist. Despite this, clinicians are actively engaged in screening adolescent dancers using a variety of methods. Even if a standardized screen were to exist for this population, there are often barriers to screening that contribute to the lack of consistency and utilization of screening including cost, time, and insufficient resources. Additionally, there is little to no research detailing the development and implementation of a screen to inform the process for other interested clinicians. Therefore, the primary purpose of this study was to develop and describe a standardized, feasible, evidence-based, clinically relevant screen and monitor injuries in adolescent pre-professional dancers. The secondary aim was to utilize the screen to identify impairments and make individualized wellness recommendations in an effort to reduce risk of injury and improve dance performance.
MATERIALS AND METHODS
Development of the Adolescent Dancer Screen
Experienced physical therapists currently conducting screens with adolescent dancers were identified through the Performing Arts Special Interest Group (PASIG) of the American Physical Therapy Association (APTA) Academy of Orthopaedic Physical Therapy (AOPT). Practitioners provided information regarding their screening methods including three published screens1,27,28 and eight non-published screens. The majority of screens included survey questions addressing dance history, personal demographics, health history, and current complaints. Fewer screens included extrinsic risks, lifestyle habits, health management and/or a psychological screen. The majority of the screens included physical measurements of lower extremity strength, orthopedic tests, functional capacity, range of motion, technique assessment, structure/alignment, flexibility, static balance, posture, core strength, and anthropometric measures. Less of the screens included aerobic fitness, standing “turnout,” gait analysis, joint laxity, pointe readiness, and/or disability severity. The Columbia Adolescent Dancer Screen (CADS) was developed by combining screening elements from the existing screens, augmenting each component with operational definitions and photos to help standardize the protocol. Every effort was made to include screening components with data on reliability and validity. Where there were gaps in the literature, efforts were made to determine reliability. Screening was completed with two cohorts of adolescent dancers.
Columbia Adolescent Dancer Screen (CADS) Components
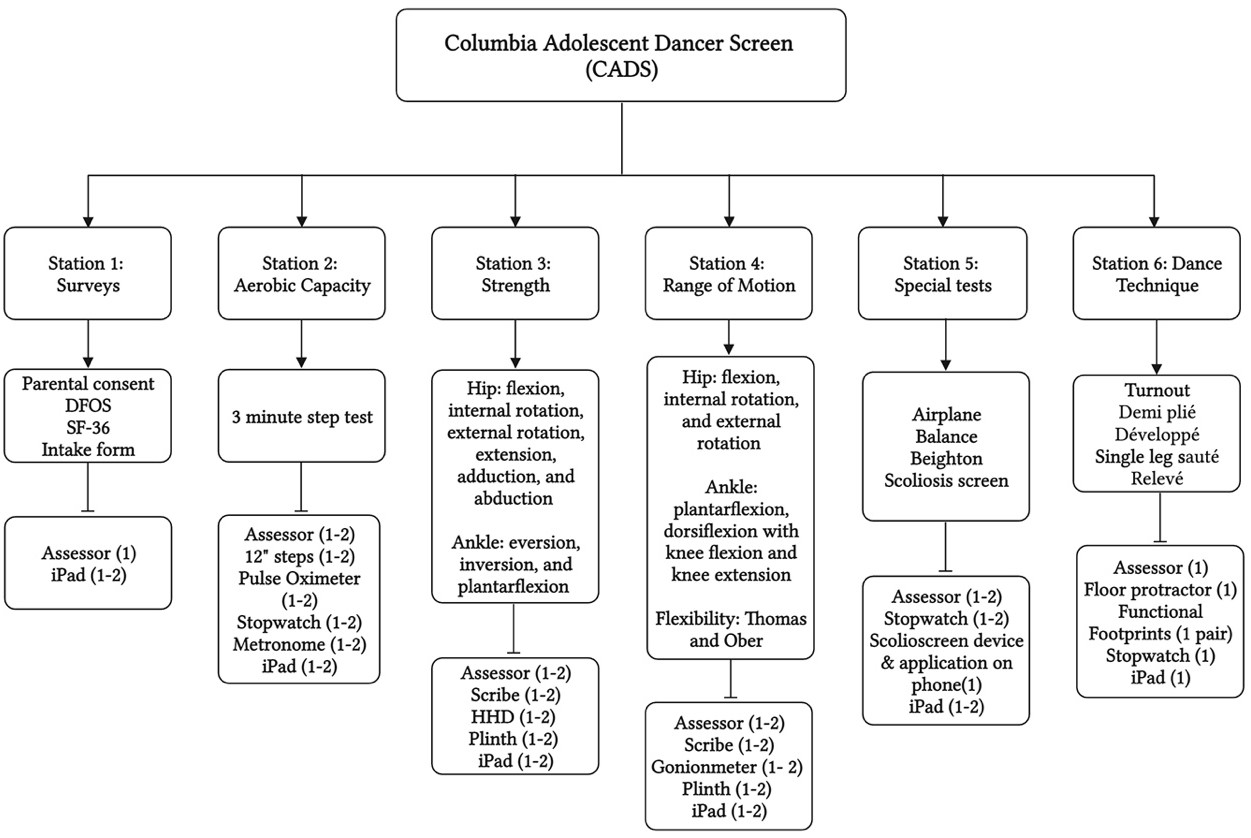
The CADS included an intake form with three self-reported outcome measures along with five physical assessment stations. These stations included aerobic capacity, range of motion, strength testing with handheld dynamometry (HHD), orthopedic special tests, and dance technique assessment.
.jpeg)
Surveys/Outcome Measures
A number of outcome measures were utilized to gather baseline data. Dancers completed an intake form with demographics including age, menstruation status, dance hours per week, and injury history. Dancers were surveyed about their eating habits including feelings regarding body image and weight via the Eating Attitudes Test (EAT-26), a self-report tool used to screen for characteristics and symptoms associated with eating disorders.29–31 Guardians were contacted for referral for potential disordered eating in any participants with EAT-26 scores over 20. Participants completed the 36-Item Short-Form Health Survey (SF-36) as an indicator of quality-of-life and general health status.32 The Dance Functional Outcome Survey (DFOS) was also included, as it is a valid dance specific self-report questionnaire with excellent reliability in pediatric dancers that is sensitive to change in healthy and injured ballet and modern dancers.33(p20),34
Aerobic Capacity
An adapted 3 Minute Step Test at 112 beats per minute was used to measure aerobic capacity, as it has been shown to be an acceptable measure for aerobic capacity in dancers.35,36 Three heart rates (HR) were recorded: resting, peak, and recovery using a pulse oximeter. Resting HR was recorded after sitting for two minutes. Peak HR was recorded after participants stepped onto a 12 inch step with alternating feet to the beat of a metronome (112 beats per minute) for three minutes. Recovery HR was recorded after one minute of seated rest.
Strength Testing with Dynamometry
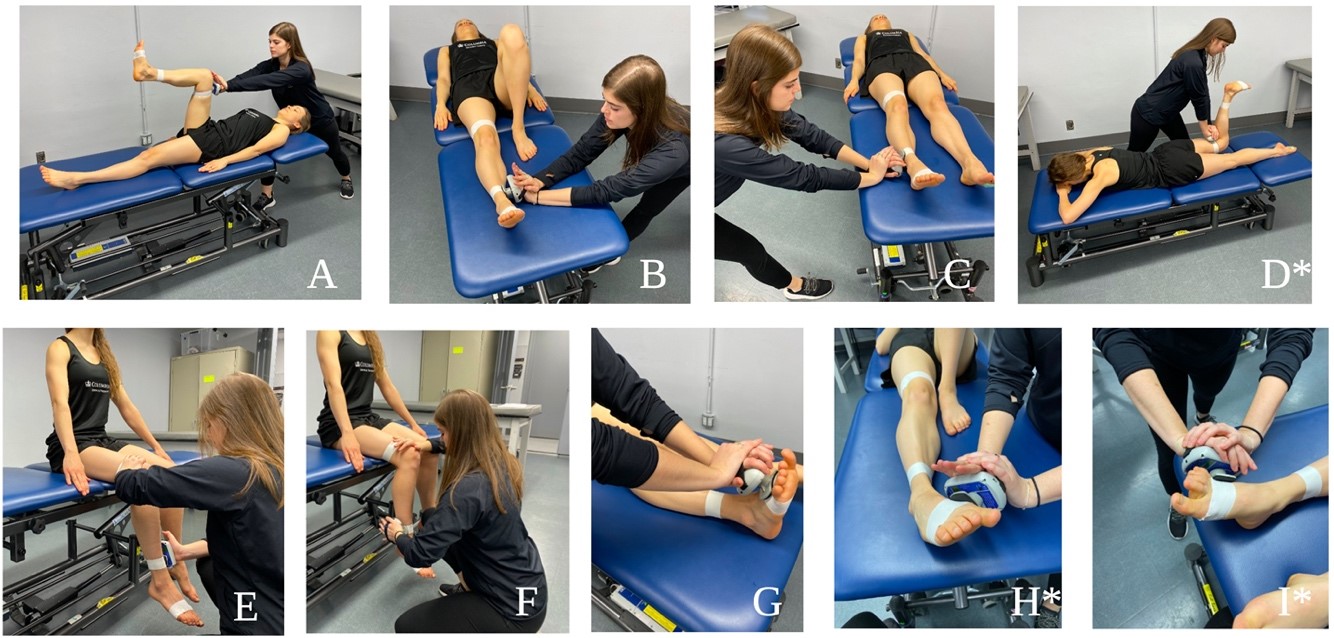
Strength testing for lower extremity muscles was completed as described by Bohannon, Alfuth, and Richardson using HHD with a single trial for each muscle group.37–39 All data were recorded in pounds. In an effort to establish reliability of HHD in pre-professional dancers, an adjunct study was performed following the initial implementation of the screen; the results of which informed updates for future screen iterations.40

Range of Motion
Joint range of motion of the hip, knee, and ankle were measured using a goniometer, following protocols established by Norkin & White.41 A single measurement was taken and recorded bilaterally in degrees for hip flexion, hip internal and external rotation, ankle plantarflexion, and ankle dorsiflexion with the knee flexed and extended.

Orthopedic Special Tests
A number of special tests were included to screen for flexibility, balance, motor control, joint hypermobility, and scoliosis. Both the Thomas and Ober tests were utilized for muscle flexibility. The Thomas Test, described by Norkin and White,41 was administered to assess iliopsoas and rectus femoris muscle length. The Ober Test, described by Norkin and White,41 was administered to assess tensor fascia lata/iliotibial band length.
The dancers were screened for scoliosis using the scolioscreen device and smartphone application.42 Dancers were positioned in standing with feet parallel and hip-width apart. They were instructed to perform trunk forward flexion by tucking the chin. The scolioscreen device was centered over the spinous processes as close as possible to the base of the spine. The examiner moved the device up the spine keeping it centered over the spinous processes and recorded the largest angle found. This process was repeated and the average of the two largest angles was recorded.
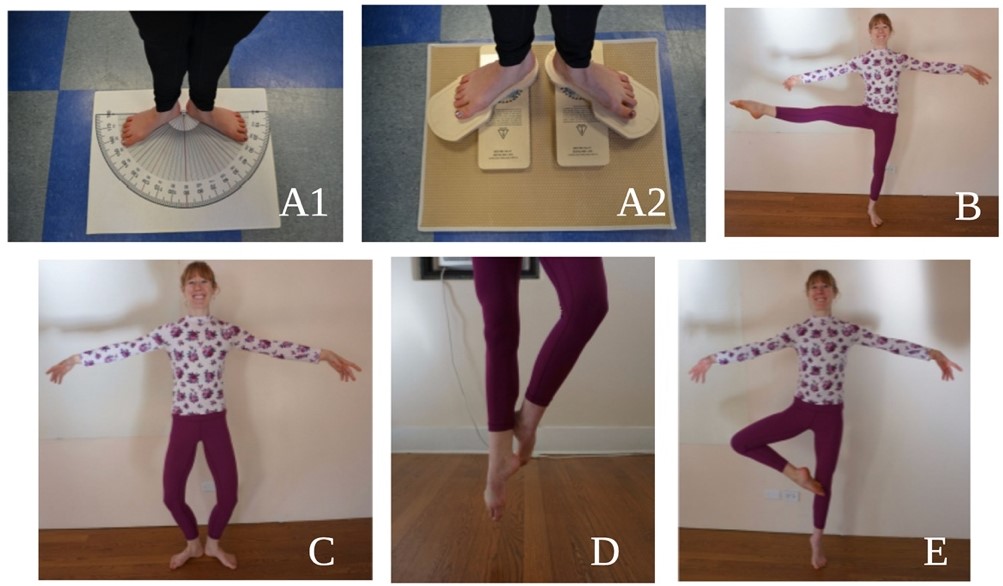
The airplane test39 was administered to assess motor control and coordination. Dancers were instructed to hinge from the hips so the trunk is near parallel to the ground, and to extend one leg back so it is also parallel to the ground. Dancers were required to maintain parallel with both legs (no internal or external rotation). To pass the airplane test, the dancer must complete four out of five pliés while bringing the arms together to touch fingertips to the ground without loss of balance or technical fault (knee over the center of the foot, maintenance of level pelvis with the foot, back, and head in one line, and no foot pronation).

Joint laxity and hypermobility were assessed by the Beighton nine point scale.43,44 A higher score indicated an increase in laxity, with six out of nine being the cut-off recommended for consideration of generalized joint hypermobility.43 Balance was evaluated by a thirty second, eyes open and closed, single leg stance test for both sides.
Dance Technique
Five dance technique items were simultaneously screened by three independent raters in the first cohort in an effort to determine inter-rater reliability. Training consisted of reviewing a manual detailing the scoring items and what constituted a pass/fail or violation of appropriate technique as well as a video practice session. Only one rater was used in the second cohort but the procedures for scoring, viewing, and number of repetitions for each technique assessment were updated following a preliminary investigation of inter-rater reliability for the screen. Each dancer was instructed to “maintain your best technique.” Turnout was measured in degrees with dancers standing in first position on a floor protractor,45 which was then compared to technically correct turnout measured in degrees using functional footprints. The other technique items were demi plié in first position, développé a la seconde, single leg sauté test,39 and relevé in retiré. Each had five to seven criteria for proper alignment of the pelvis, trunk, and lower extremities that were evaluated and recorded.

Individualized Wellness Recommendations
After dancers completed the screen, their results were reviewed for any flagged criteria by the SPTs on the dance research team with oversight by licensed clinicians to provide targeted exercises and stretches to address potential deficits found during the screen. All the guidelines included patient education materials sourced from IADMS and the American Ballet Theatre website.

Implementing the Adolescent Dancer Screen
Training
In order to implement the screen, it was necessary to create a training manual and orient team members to screening items. A brief team meeting oriented team members to the screen. Technique assessors did an extra one hour training with videos and discussion. This was followed by an hour-long practice session for student physical therapists (SPTs) participating in the screen, SPTs with volunteers that allowed team members to practice performing their station assessment three to five times.
Participants
Participants included two cohorts of 32 female adolescent dancers, mean age of 14 (range 11-17), from two different dance studios’ pre-professional programs surveyed a year apart. All participants gave informed consent, and the study was approved by the institutional review board. The participants had to be between the ages of 10 and 19, taking a minimum of two ballet classes per week. Dancers were recruited via flyers at both studios and all dancers assented to study participation with verbal and written consent. As the majority of dancers were minors, verbal and written consent were also secured from parents/guardians prior to screening. Screenings took place at the dance studios.
Screening Day
Dancers signed up to participate in advance of the screening day for both cohorts. For cohort one, dancers were told to come in between rehearsals while dancers in cohort two were given a scheduled time to arrive with four dancers scheduled every 30 minutes. Ten minutes were allocated to each of the six screening stations - five physical assessment stations and one paperwork station. Prior to screening, folders and participant numbers were created for each dancer that included intake paperwork as well as a form to record results of each station. This was done electronically with iPads for cohort two.
In cohort one, the six station set-up for the CADS included nine assessors with two additional raters at the technique station to evaluate reliability. A single dance studio (~30’ x 25’) was able to accommodate all stations with assessors and up to six dancers at a time. The studio was reserved for three hours (including setup) to screen a maximum of 20 dancers. The results were collected via paper and pencil on a clipboard that each participant carried with them from station to station.
In cohort two, a small studio (~20’ x 30’) was used. Nine assessors were again present with one additional team member operating in capacity as a coordinator to oversee the process, direct dancers, and remedy any consent issues. Only one assessor was present at the technique station, but assessors were utilized as scribes for both the range of motion and strength testing stations.
Post Screening
Following screening, each dancer was contacted via email for 14 weeks to fill out a survey on injury surveillance that could be completed in ten minutes or less. The surveys were sent using REDCap, a HIPAA compliant database and data collection system. The online survey (modified Oslo Sports Trauma Research Centre’s Questionnaire on Health Problems) used three definitions for dance-related injuries: (1) time loss (an inability to complete one or more classes, rehearsals, or performances for one or more days beyond onset), (2) medical attention, and (3) any complaint.46 Additionally, the SPTs with clinician oversight provided each dancer with an individualized wellness recommendation packet based on their screening findings.
RESULTS
Two screening days were completed with two cohorts, one of 17 and one of 15 dancers. Data collected from both cohorts is reported in Table 2. Data from cohort one technique inter-rater reliability is reported in Table 3. Screen feasibility was assessed in four categories: practicality, demand, implementation, and adaption.47
Practicality: Efficiency and Cost
As a measure of efficiency, the team was able to streamline screening from five to six dancers per hour (cohort one) to seven to eight dancers per hour (cohort two). The cost of screening can be evaluated in personnel, time, and equipment. Nine assessors administered the screen to each cohort, although as few as six would be able to run the screen. The time commitment of an hour from each dancer was accurate and sufficient to allow for screen completion. A time commitment of 3-4.5 hours was necessary from SPT assessors, although licensed physical therapists were able to run stations without a practice session and just a 30-minute orientation, lessening their time commitment to 2-3.5 hours. Equipment costs were kept to a minimum where possible and portable, space-efficient equipment was prioritized. The hand-held dynamometer, approximately 800 dollars, was the largest expense; two were utilized to improve efficiency. The remaining equipment items could be purchased for roughly 500 dollars (for the full list of equipment refer to Figure 1).
Demand: Screening Utilization
All available screening slots for both cohorts were filled with all dancers agreeing to be subsequently surveyed for injury, indicating high demand for screening in the sample populations.
Implementation: Factors, Successes, and Failures
A number of factors affected implementation, including the need for parental consent with an adolescent population. Another factor associated with implementation was adequately training SPTs to perform the screening. With a robust training manual, orientation, and practice session, all team members were able to successfully conduct the screen regardless of dance experience. Some failures experienced in cohort one included dancers missing stations, bottlenecks that slowed dancers progress through stations, and having to manually enter data from paper to an electronic format introducing opportunities for error and decreased efficiency.
Adaptation: Performing the Screen on a Second Cohort
In cohort one, 17 dancers were assessed in a three-hour block with two dancers missing station one and one dancer missing a portion of the technique station due to scheduling conflicts and bottlenecks at the warm up and special tests stations. Changes and updates for cohort two allowed all dancers to complete all the stations and increased the number of dancers screened per hour.
DISCUSSION
The CADS was developed and successfully implemented across two cohorts of 32 adolescent dancers. The screen is feasible, practical, and satisfies demand. The screenings collected baseline measures, informed wellness recommendations, and established positive contact between dancers and medical professionals. The purpose of this investigation was twofold, involving both development and implementation.
Screen Development
A combination of personal contact with authors of current professional dancer screens and literature reviews was conducted to find the most efficacious, valid, and reliable screening items. There are few studies that include normative data for dancers, although this is starting to change.48 It is also difficult to find screens that solely rely on measures with proven reliability. Questions around screening validity and reliability prompted thoughtful consideration of what to include in the screen. Ancillary studies were conducted in three areas where data on reliability and validity were missing: HHD in the dancer population,40 inter-rater reliability of the technique screen,20 and the relationship of compensated turnout with injury.49,50 Subsequent studies have shown a similar technique screen and turnout measurement to be valid and reliable in an adult dancer population.51,52
Substantial time and effort were invested in creating a thorough training manual, a database of questionnaires and forms, and developing wellness recommendations based on screening results. Limited normative data and literature on risk factors associated with injury prompted inquiry into how to identify criteria for prescriptive wellness recommendations. In a population just starting to develop normative data,48 what thresholds should be utilized to signal a need for attention? Furthermore, questions were raised about the necessity of collecting multiple data points on a large number of individual muscle groups when cardinal muscle groups could potentially be used to streamline the process.53 Ultimately wellness recommendations were given for large asymmetries in strength or flexibility, positive orthopedic special tests, and for multiple errors on technique screening items. These individualized recommendations were sent in the weeks following the screening. While the recommendations were meaningful to the dancers and helped incentivize screening participation, providing more immediate results may elicit greater response rates for follow up injury surveillance surveys in the future.54
The importance of building a pool of normative data along with the continued study of links between injury risk factors and screening continue to be a priority. Since developing the CADS, Critchley et al.48 developed and conducted a preseason screen and subsequent weekly survey for over 450 pre-professional dancers over a 5-year period. Their screen included many of the same mobility and strength assessments as CADS, and their survey yielded a 91.4% response rate. Results identified dynamic balance assessments and years of training as potential protective factors against self-reported injury.48 Critchley et. al. support the feasibility of a screen like CADS, but it also underlines the importance of including a valid, population-specific assessment of movement quality.48
Screen Implementation
The team found it was efficacious to partner with local studios to use their space and schedule screenings when dancers were already at the studio. In the adolescent population, special consideration is needed as the dancers depend on their parents for transportation, scheduling, and consent, which involves a more proactive approach. In the team’s experience, obtaining parental consent was best achieved by someone who already had a relationship with the studio. Alternately, where a relationship needed to be created, hosting a wellness workshop to engage dancers in the importance of injury prevention prior to the screening day helped establish a relationship and gave dancers/parents a chance to sign up to be screened.
With the initial cohort, the team found inefficiencies and opportunities for improvement that were streamlined for the second screening. In cohort one, the largest bottleneck was at the warm up station, as that station had to be completed first. To remedy this, another aerobic step station was added for cohort two. The other congestion point was at the orthopedic special tests station. Delays were removed by moving the two orthopedic special tests that required a plinth (Thomas and Ober) to the ROM station. The most time consuming station was HHD; in cohort two an additional plinth and assessor were added to this station which improved efficiency. Another cumbersome and time consuming aspect of the initial cohort was the need for stabilization belts. Subsequently HHD has been shown to be reliable in a dancer population without the need for stabilization belts,40 therefore, they were not utilized in the second cohort, which decreased time required for testing. Through experience with the ancillary HHD study,40 the use of printed photos of positions at the station helped decrease errors of HHD placement and cognitive effort required by the assessor, also improving efficiency. In the original cohort, there were three testers at the technique station in order to obtain data on reliability, as none existed at the time. The second cohort required only one tester, which allowed for personnel to be utilized as scribes for the flexibility and HHD stations, again improving efficiency.
Following assessment of inter-rater reliability of the technique screen, additional training was added for the second cohort in an effort to increase reliability, including an additional one hour practice session with videos and discussion to become familiar with the screening tool and common errors. Procedures for scoring, viewing, and number of repetitions were updated in an effort to improve reliability, although the results of these updates have yet to be analyzed.
With cohort one, the dancers carried paper documents from station to station for assessors to fill out, which required the data to later be transitioned from paper to computer format. In the second cohort, the use of iPads helped to improve efficiency for concurrent data entry at each station, decreasing error potential. While most dancers were dressed in leotards and tights, it became apparent after cohort one that dress code instructions were needed to avoid instances of clothing hindering accurate assessment of lower extremity positions and alignment. Because cohort one had dancers that failed to complete all stations, adding a floating assessor who could oversee operations, act as another assessor if needed, and check each participant’s electronic record to ensure all stations were completed worked well; every dancer in cohort two completed every station. Finally, as part of post-screening injury surveillance data was collected with preliminary data showing heterogenity and requiring a larger “n” to draw meaningful conclusions. However, as this was not a primary purpose of this study, results of the injury surveillance are not reported in this paper.
Limitations
The CADS has been piloted with two cohorts with less than twenty dancers in each cohort and has not been tested in larger cohorts, however, the authors’ anticipate carryover in larger groups. The CADS follow-up injury surveillance was also limited to 14 weeks with analysis of that data ongoing. Although efforts were made to include reliable screening elements or to establish reliability, validity and predictive capabilities also need to be established. In this iteration, the main purpose of screening was to identify impairments from screen results to inform wellness recommendations in an effort to reduce injury risk and improve performance. While reliability for HHD has been shown for the lower extremity in dancers,40 the CADS technique station reliability ranged from poor to excellent20 and efforts to improve reliability still need to be evaluated statistically. In addition, the two cohorts were demographically similar but differed in hours danced per week, which indicates variation in training levels. While this did not change the contents of the screen or how it was administered, literature has shown increased dance hours to be associated with injury.16,55 This makes positive association with healthcare professionals, a secondary benefit of screening, even more important.
CONCLUSION
Adolescent dancers are a population that frequently experience injury and have a real need for injury surveillance and screening. There are a number of potential barriers to screening, however the results of this study indicate that the CADS is a feasible screen that overcomes barriers by being pragmatic, evidence-based, and efficient. Screening can be used to establish dancer baseline data, provide the dancer with informed wellness recommendations, and serve as a positive introduction for adolescent dancers to medical professionals.
Conflicts of interest
The authors report no conflicts of interest. All figures were created with BioRender.com
ACKNOWLEDGEMENTS
Nunnbetter Dance Theater & Dance for Joy
Sunny Bjaanes, Marissa Schaeffer, Sarah Edery-Altas, & Demetri Dimitriadis
Hilary Busick, Aimee Fries, Allison Ventola, Margaret Bryant, & Shalomit Mikhaylov
Lindsay Backiev, Mandy Blackmon, Shaw Bronner, Maribeth Crupi, Erin Hayden, Tessa Kasmar, Michelina Cassella Kulak, Marijeanne Liederbach, Tiffany Marulli, Duane Scotti, & Jennifer Stoskus