

BACKGROUND
Hamstring injuries are frequent and occur in many different sports.1 Furthermore, relative to other injuries, hamstring injuries are the most common recurrent injury in football (soccer) and typically leads to longer absence from the sport than the initial injury.2 Injuries can range from acute tears of the hamstring muscle to overuse related injuries to the proximal and distal tendons. Several factors are thought to elevate the risk of hamstring injuries including high-speed running, previous hamstring injury and lower muscle strength.3
A recent systematic review and meta-analysis indicated that isometric side-to-side strength deficits after an acute hamstring injury may settle within 20-50 days, but the isokinetic strength deficits can remain even after return to play.4 Of note, Tyler et al. have been shown that moderate side-to-side strength deficits in isometric peak torque may be muscle length dependent when they demonstrated that isometric strength deficit of the knee flexors were more evident at longer muscle lengths.5 Furthermore, the athletes who adhered to their specific program fully recovered their hamstring strength at long length and had no re-injuries after returning to high-speed sports compared to those who did not adhere. Collectively, these findings suggests that a strength deficit after hamstring strain at long muscle length should be addressed during rehabilitation.6 Similarly, athletes with hamstring tendinopathy may also benefit from knee flexion strengthening at lengths.7 Testing strength at longer muscle length may reflect the larger work of the hamstring at the late swing phase and initial contact with the ground during running.8
Evaluation of hamstring strength in research and clinical practice is important and has been extensively investigated.4 While isokinetic testing is considered the gold standard and has been shown to be a valid and reliable in testing method for hamstring strength, it is expensive and can be impractical.9 Hand-held dynamometry (HHD) is a relatively inexpensive and practical alternative to isokinetic strength testing. Moderate to high correlation between isokinetic testing values of the hamstring muscles and those obtained with HHD has been described.9 The testing position in the isokinetic machine in a lengthened position could be mimicked with a hand-held dynamometer as proposed by Schmitt, Tyler, and McHugh.10
Methods
Participants
Twenty healthy active participants were recruited at Bispebjerg Hospital in Copenhagen. They were recruited using convenience sampling, meaning participants were employed by departments of the hospital or were from local sporting clubs. The activity level of the participants ranged from recreational running to elite level track and field. Inclusion criteria: No pain in the hamstring, gluteal-, groin- or gastrocnemius musculature in the prior three months. Likewise, no pain in the back, knee- or hip joint was allowed. Previous hamstring strain was not an exclusion criteria (beyond the three-month pain free criteria) as any strength deficits would theoretically have presented on all tests. All participants received written information prior to participation and gave written consent for participation before testing. All participants were measured in height and weight on test day one. Participant information is displayed in Table 1. No approval from the ethical committee of the Capitol Region in Denmark was necessary due the non-invasive nature of the testing procedure.

Isometric Strength Testing using the Biodex
The participants performed a 10-minute warm up on a stationary bike at a self-selected intensity. The Biodex was adjusted so the participants were seated with approximately 45 degrees of hip flexion (measured with a goniometer) above the horizontal plane and with an 85-degree upright back position. The participants were strapped to the machine across the torso and the hips, and the testing limb was fixated. The axis of rotation was aligned with the femoral condyle. The participant then maximally extended the knee, and the lever arm was fixed in this position (Figure 1). In this position the participants were allowed to do two familiarization attempts (75% subjective MVC) before the test began. Once the test procedure was initiated the participants executed three maximal knee flexion isometric contractions for 5 seconds with 30 seconds of rest in between contractions. This was repeated on both legs (starting with the right leg). The highest value of the three attempts was used for analysis and converted to newton using this equation The conversion was done to be able to compare the values with the HHD, which measured Force.

Isometric End Range Hamstring Test with Handheld Dynamometer
To conduct this test, the participants were placed in supine and pulled the thigh of the tested leg into maximal hip flexion with their own hands. The contralateral leg was in a neutral position and fixed to the table via a belt strap as shown in Figure 2. The tester was positioned standing on the floor with one hand supporting and maintaining maximal hip flexion of the participant. One the arm that held the HHD, the elbow and arm was locked to the tester’s torso. This was done to ensure that the entire body, and not just the upper limb, withstood the force from the participant. The participant then actively extended the knee joint maximally and the tester placed the dynamometer (Lafeytte HHD, model 01165A) on the calcaneus and the subject performed an isometric knee flexion contraction which was held for three to five seconds. The participants were instructed to maximally bend the knee and the tester initiated the test by saying: "Ready, set, go" and provided encouragement by saying: “push, push, push and relax”. This was repeated three times on each side with 30 seconds of rest in between contractions. The highest value of the three tests were used for analysis. Force in kg was multiplied by 9.81 to convert to Newton and compare with Biodex values.

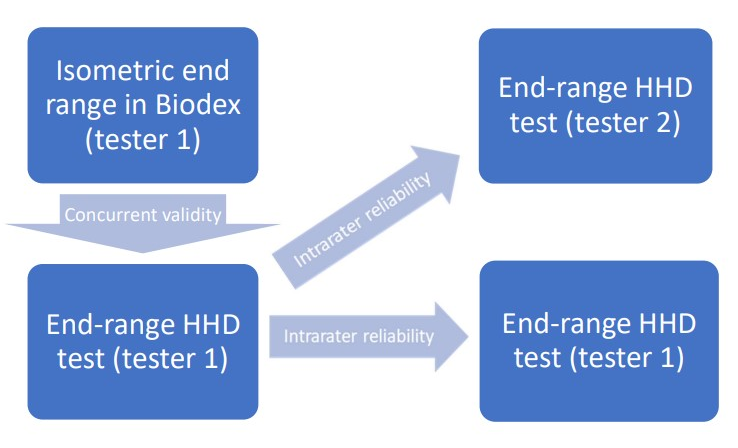
Test Flowchart
The participants were tested on “Test Day 1” and re-tested approximately 7-10 days later at “Test Day 2” (Figure 3). On “Test Day 1” the participants were tested in the Biodex machine by Tester one after a 10-minute warmup on a stationary bike. Once the Biodex testing was completed, participants were allowed to rest for ten minutes. After the 10 minutes the isometric end-range hamstring test with HHD by Tester one was executed.

Seven to ten days later “Test Day 2” was scheduled. The time between testing was chosen from a convenience perspective, where both testers were able to attend at the same time. The participants again performed a 10-minute warm up on the stationary bike before the isometric end range hamstring test with HHD was performed by Tester two. Participant were once again allowed a 10-minute break before the test was repeated by Tester one in a different room.
This setup enabled measurement of the intratester reliability between Day 1 and Day 2 with measurements taken by Tester one. The two testing sessions on Day 2 enabled measurement intertester reliability between Tester one and Tester two. Tester one was a male with extensive experience with the use of a handheld dynamometer whereas Tester two was female with little experience with HHD.
STATISTICAL ANALYSIS
Pearson product-moment correlation coefficient was used to determine the validity of the HHD test in comparison to the Biodex machine. Bland-Altman’s plots with limits of agreement (LOA) were used to visually address the potential systematic bias between the two testing methods. The between-session mean differences were investigated using a paired t-test, to assess the systematic bias between the two days of testing. The relative intra- and inter reliability was tested using an Intraclass correlation Coefficient (Two-way random, single score, consistency definition). Absolute intra- and inter reliability was calculated Standard Error of Measurement (SEM), which was expressed as: Standard Deviation_pooled x This was also calculated as a percentage (SEM%): Level of significance was set at p < 0.05. All statistical analyses were performed in RStudio (4.2.2 version).
RESULTS
Concurrent Validity
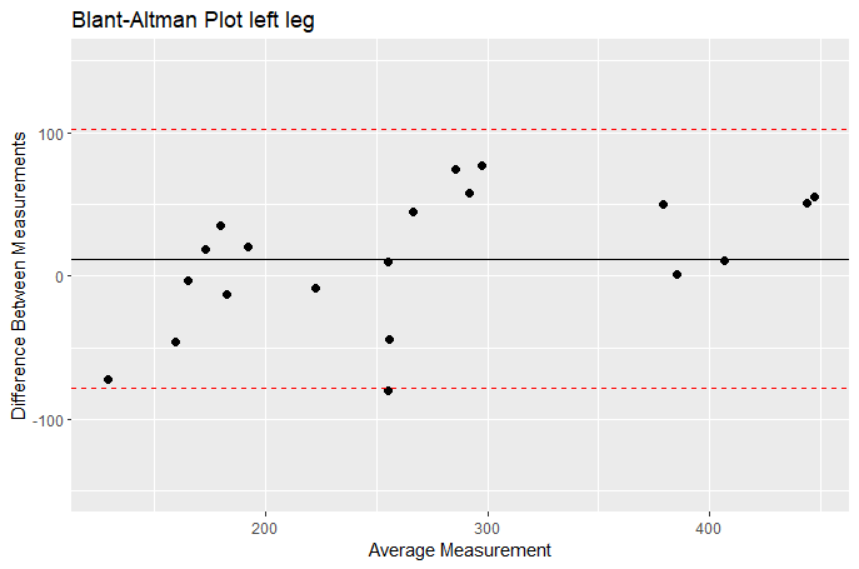
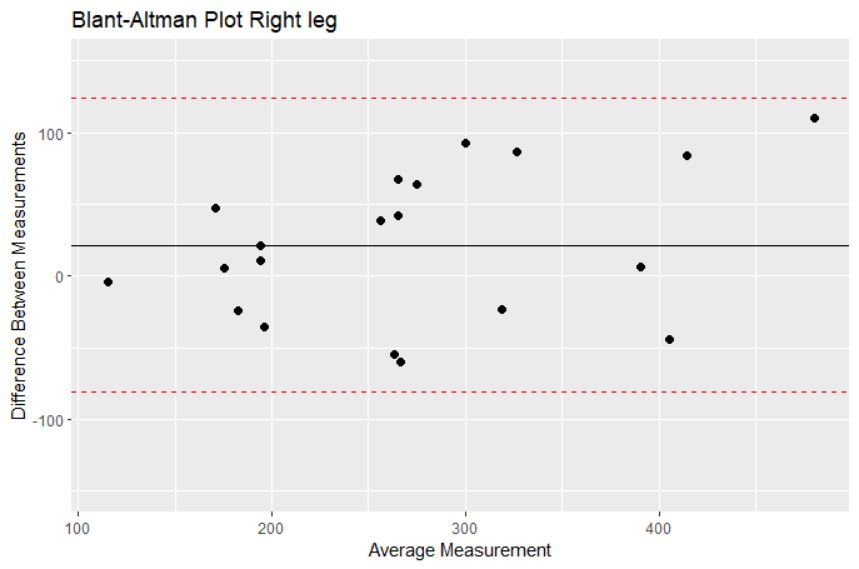
There was a significant strong correlation (Pearson’s product-moment) between strength testing in the Biodex machine and with the handheld dynamometer on both the right (r= 0.87, p < 0.0001) and left side (r= 0.911, p< 0.0001). The Bland-Altman plots (Figures 4 and 5) show that all the datapoints are within the levels of agreement and the mean difference between the two measurements lie between 12 N for the left leg and 22 N on the right leg, which clinically would be seen as a small difference between the two measurement instruments.


Reliability
There was no systematic bias between any of the dynamometer tests, with respect to separate test days and testers. The relative intratester reliability between the two test days was excellent and the absolute reliability (SEM%) was 8.5 % for the right and 8.2 % for the left leg. Relative interrater reliability for the right leg showed good reliability (ICC=0.83), whereas reliability for the left leg only showed moderate reliability (ICC= 0.71). The absolute interrater reliability (SEM%) was 11.2 % and 16.1 % for right and left leg respectively. Inter- and intra-rater reliability results are shown in Table 2.
DISCUSSION
The main findings of this study were that a standardized end range hamstring muscle strength test with a hand-held dynamometer is a valid measurement compared to isokinetic testing. The data also show excellent intra-rater reliability (ICC > 0.9) and moderate to good inter-rater reliability (left ICC = 0.5-0.75, right ICC > 0.75). Furthermore, the absolute reliability, SEM < 10 % for intra-rater and SEM < 17.2 % for inter-rater shows that this simple test can be used to measure knee flexor strength with acceptable measurement error.11
The current study evaluated knee flexor strength in a lengthened position with the hip flexed at 45 degrees relative to the horizontal plane and the knee in maximal extension. This position places the knee flexors under considerably more tension than other commonly used positions for evaluating knee flexion strength, such as a seated isokinetic testing and prone position with 0 degrees of hip flexion and 15 degrees of knee flexion.4,12 Despite the potential instability of this position, the current study found excellent intra-rater reliability (ICC > 0.9) and moderate to good inter-rater reliability (left ICC = 0.5-0.75, right ICC > 0.75), with low standard error of measurement (SEM < 10 % for intra-rater and SEM < 16.1 % for inter-rater). The difference in ICC’s for the left and right leg may be due to the fact that tester 1 was a lefthanded male whereas tester 2 was a righthanded female. This means that tester 2 might have had difficulties maintaining the same level of force when testing the left leg compared to the right leg, thereby seeing poorer reliability.
The study suggests that the evaluation of isometric hamstring strength in this lengthened position can be reliably performed in clinical practice and research, particularly if the same person repeats the testing procedure.
The current study found excellent intra-rater reliability and moderate to good inter-rater reliability for the end-range hamstring strength test with a hand-held dynamometer. This is consistent with previous studies that have used hand-held dynamometry to measure hamstring strength in a seated or prone position with 0-15 degrees of knee flexion. For example, van der Made et al. found good inter-tester reliability (ICC 0.80-0.87) when testing high-level rugby players in both prone and seated positions, while Larsson et al. found good intra-rater reliability in a prone position with 0 degrees of hip flexion and 90 degrees of knee flexion.12,13 The current study also showed moderate to good inter-rater reliability despite the testing position being considered less stable and the two testers being of different sex and presumably upper body strength. These findings suggest that the end-range hamstring strength test can be reliably performed by different testers in clinical practice and research.
The results of this study showed strong correlation (concurrent validity) between isometric hamstring strength testing with the HHD and Biodex in the lengthened position. This is consistant with Mentiplay et al. who also showed good reliability (ICC= 0.79-0.87) and strong correlation (r=0.66-0.76) when comparing HHD with isometric knee flexor strength using a KinCom isokinetic machine.14 The testing was done in seated position with 90 degrees of hip and knee flexion while the tester had the arm on the wall for support. Even though this would be considered a much more stable testing position for both the tester and participants, the current study shows good correlation and agreement between HHD and the Biodex in this lengthened and more difficult testing position. This implies that testing knee flexor strength in this lengthened position with HHD is valid and useful in clinical practice and in research.
The results of the current study suggest that assessing knee flexor strength in a lengthened position with handheld dynamometry can be a useful tool for monitoring rehabilitation in a more functionally relevant position. A recent systematic review by Manier et al. showed a normalization of knee flexor strength deficits at longer lengths before returning to play, while Nara et al. measured a decrease in isometric knee flexor strength after returning to play following hamstring strain.4,6 The first study analyzed strength at longer lengths at 0 degrees of hip flexion and 0-15 degrees of knee flexion. This is far from the length that was used by the later study (85 degrees of hip flexion and 30 degrees of knee flexion). Although a smaller study, Nara et al.6 may have measured knee flexion strengths at a more relevant position of the hamstrings during sprinting, which could be the reason for the detection of the strength deficit. The current study placed the knee flexors under considerably more tension than other commonly used positions for evaluating knee flexion strength, which could be an alternative way of measuring knee flexor strength and detecting deficits before and after returning to play. This could be particularly useful for targeting rehabilitation with an emphasis on eccentric training at longer lengths, as suggested by Tyler et al.5 Others have shown that hamstring strength at longer lengths is more representative of rehabilitation progression than strength at mid-range (0 degrees of hip flexion and 30 degrees of knee flexion) and inner-range strength (0 degrees of hip flexion and 90 degrees of knee flexion).11 Given the fact that the lengthened testing position is valid and reliably measured with the HHD, such a measure would also be more practical and less costly than isokinetic testing in a clinical setting.
Limitations
There are some limitations that deserve consideration. Firstly, the Bland-Altman plots revealed a potential for heteroscedasticity, indicating that there may be a tendency for larger differences between the HHD and the Biodex measurements in subjects with higher force production. This suggests that the agreement between the two methods may vary depending on the individual’s strength level. The decision was made not to use external fixation, such as a strap fixated to the wall, during the testing procedure. Pilot testing revealed that the lengthened testing position used in this study required more training for the testers compared to other commonly used positions for evaluating knee flexion strength. This may have introduced some variability in the measurements and could affect the reliability of the results. However, this makes the testing procedure much more practical than with the use of external fixation (for example to the wall). Hand dominance and tester strength were also not considered and may have added to the variability. Additionally, there was no blinding between the results of the isokinetic testing and the subsequent HHD measurement on the first day of testing. Tester 1 conducted both tests, raising the possibility of result memorization from the Biodex affecting the HHD measurements. To minimize this potential bias, the authors took precautions by recording the results from the Biodex and the HHD on different measurement systems. The Biodex results were written down by hand on a piece of paper, while the HHD testing was carried out and the results were recorded on a different sheet. All the results were then entered into a spreadsheet for calculations. Although not formally blinded, it is unlikely that the tester could memorize and calculate the values, thus minimizing the impact on the HHD testing results. The decision not to blind the comparison between isokinetic testing and HHD on the first day of testing was made due to the unavailability of Tester 2, who could only attend the testing sessions on subsequent days.
CONCLUSION
The results of the current study indicate that assessing knee flexor strength in a lengthened position with handheld dynamometry can be done with excellent intra-rater reliability and moderate to good inter-rater reliability, with standard error of measurements below 10 % and 20 %, respectively. This assessment shows strong correlation with isokinetic strength testing, considered the gold standard. The end-range hamstring strength test can be utilized in research and clinical settings to determine knee flexor strength in a more functionally relevant position than usual test positions with HHD.