INTRODUCTION
Injuries to the upper extremity in baseball pitchers continue to rise across all levels of play.1–4 Many shoulder and elbow injuries - such as injuries to the ulnar collateral ligament (UCL), rotator cuff, and glenohumeral capsulolabral complex - often require surgical intervention and an extensive period of rehabilitation. As pitchers prepare to return to competition after these injuries, interval throwing programs (ITP) are used to progressively apply load to the healing tissue. Several ITPs have been published,5–10 with a wide variety of recommendations regarding the distances, intensities, frequency, and volume between programs.
The most widely used program in the baseball community comes from Reinold et al,10 which was published over 20 years ago. While historically this ITP has been used successfully to rehabilitate thousands of players and in a variety of published outcome studies,11–14 the development was based upon expert opinion and limited knowledge of throwing biomechanics at that time. Since its original publication, we have seen advances in our understanding of the biomechanics of throwing, as well as a better understanding of training workloads and correlation to injury risk.15 In addition, the game of baseball has evolved over the last 20 years, specifically how pitchers prepare for competition. Pitchers at all levels of play are throwing with more velocity and less downtime in an attempt to better prepare themselves throughout the season.
The concept of monitoring chronic workload and acute:chronic workload ratio (ACWR) have been popularized by Gabbett and his colleagues.16–18 ACWR is the ratio between the average daily workload over the previous 7-day bucket compared to the workload of the previous 28 days. Studies in field sports and lower extremity injuries have shown that athletes have a higher chance of injury when ACWR exceeds 1.3.19–23 In baseball, pitchers who had an ACWR of 1.27 or greater had a 14.9% higher chance of injury.23 Thus, it is important to build an ITP that progressively builds an appropriate amount of chronic workload to prepare the athlete for competition, while assuring a gradual progression of ACWR.
With a better understanding of the biomechanics of throwing, the different components of an ITP, and how to quantify training loads as throwing programs progress, a modern version of an ITP that incorporates this with the current state of baseball training is needed. It is important that an ITP reflects the needs and common practices of the modern baseball player. Therefore, the primary purpose of this paper was to create an updated ITP based on our current understanding of the biomechanics of throwing, healing of soft tissue of throwing related injuries, and the authors’ clinical experience working within baseball. This updated ITP will assure a gradual buildup of chronic workload to a desired level while staying within acceptable ACWR. The secondary purpose was to compare throwing days, chronic workload, and ACWR to projected workloads of the original ITP by Reinold et al.10 We hypothesize that the updated ITP will have a more gradual chronic workload progression while spending a larger percentage of the program within the desirable ACWR.
METHODS
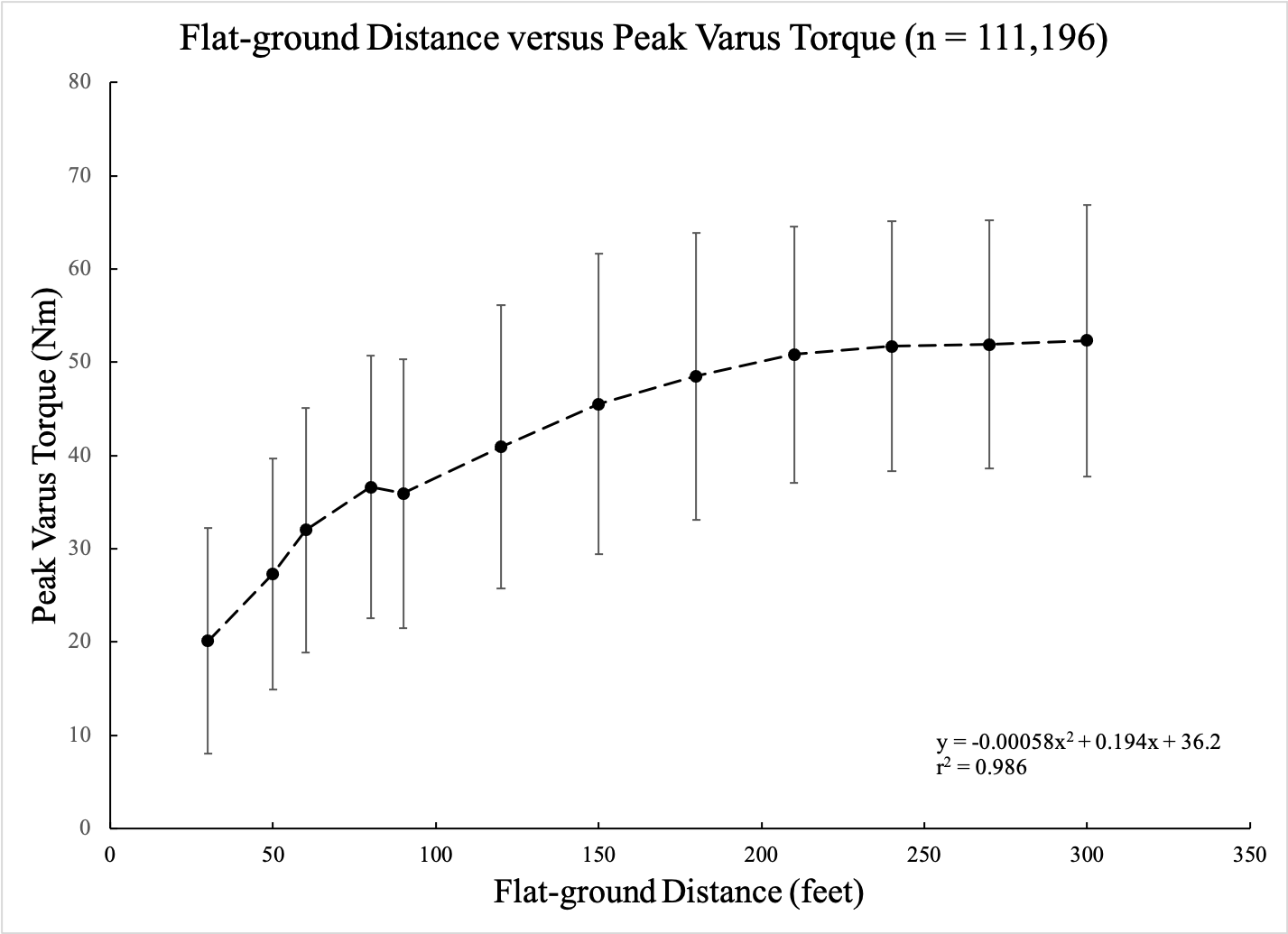
Elbow varus torque and workload for the throws in the original ITP10 were calculated using the methods and models described by Dowling et al.9 In order to determine elbow varus torque for each prescribed throw, data were mined from Motus Global’s MotusBaseball sensor (now Driveline Pulse; Driveline Baseball, Kent, WA) database. A total of 238,611 anonymized flat-ground throws were extracted from one NCAA-Division 1 team using only healthy players (n=34, 186 ± 7 cm, 89.4 ± 10.8 kg). Of these, 111,196 flat-ground throws were tagged with as ‘long-toss’ with a distance ranging from 30 ft and 300 ft. Distances with over 1,000 throws were used in the model. A 2nd order polynomial regression was created to classify a relationship between throwing distance (x in ft) and peak elbow varus torque (Nm) (Figure 1).

Development of the Updated Interval Throwing Program
An updated program was created with the goal of the program to create a safe increase in workload but also mimic a more familiar baseball throwing progression for the modern pitcher. See supplemental file for Table 1 - Long Toss ITP and Table 2 - Mound ITP. Trends in baseball training and throwing programs have progressed over the years. We wanted to make the updated program more similar to typical throwing programs being used within baseball by healthy players, and clearer by providing an exact throwing schedule with exact distances and throw counts each day. The original ITP listed ‘Phases’ and instructed pitchers to complete each phase twice before moving on, meaning the pitcher throws the exact same count and distance twice at each phase. We created the updated program to list each specific throwing day, also termed ‘Steps’, with changes in throw counts, distance, and intensity every day (or step). We also removed throw count ranges to eliminate ambiguity and varying workload.
Daily workload was the accumulation of the torque from every throw in a given day. Acute workload was calculated as a 7-day rolling average of daily load and chronic workload was calculated as a 28-day rolling average of daily load.9 Similar to Dowling et al,9 the updated program was developed to maintain an optimal ACWR while increasing the chronic workload throughout the program. The updated program started off gradually, with a pitcher throwing 30 ft. This was done to allow for a pitcher to become more confident with throwing after an injury and to slowly build chronic workload. Throwing was scheduled for 3 times a week, until Week 22. Throwing every other day with 2 days off in the these first 22 weeks has shown to keep the ACWR in check without large oscillations as seen in the original program.9 Throwing volume and throwing distance were gradually increased until 120 ft was achieved (Week 11-12). Long toss throwing included throwing with a step and an arc to allow distance to dictate the intensity, and progress to throwing on a line. Pitchers were then instructed to pitch from the flat-ground for two weeks to get reaccustomed to the pitching motion from a stationary position before progressing to the mound (Week 16).
The mound progression consisted of light and heavy flat-ground days, bullpen sessions, and light catch. Heavy load long toss days include pulldowns, with the athlete instructed to take a shuffle step and then throw with intent on a line. Fastball pitches started at 50% effort and increased to 75%, 90%, and 100%. Pitchers were allowed to start throwing change-ups in Week 19 and breaking balls in Week 23. Because the elbow varus torque observed between different pitch types has not been found to be significantly different,24–26 the percentage of different pitch types was not specifically allocated for in the program. This allowed each pitcher to individualize the program based on the types of pitches thrown.
The updated program also incorporated in ‘deload’ weeks multiple times throughout the course of the program. These weeks were programmed in at 4 spaced out times, at Weeks 7, 14, 22, and 29. Deload weeks consisted of light throwing only and each deload week was different throughout the program in order to keep the ACWR near the low end of the desired range.
Workloads for the Original ITP
Workloads (i.e. daily, acute, chronic, and ACWR) for the original ITP were built from the prescribed throwing schedule. The original ITP instructed pitchers to throw every other day and perform each phase 2 times before advancing to the next phase. Warm-up throws were prescribed at 30-45 ft and then to progress to the designated distance. To account for this, warm-up throws were codified with 5 throws at each distance starting at 30 ft and progressing 15 ft (45 ft distance) and then 30 ft after that to the prescribed throwing distance for that day. The original ITP had specific throw counts for each distance until 75 ft, and then provided ranges at each distance after that (i.e. 75 ft 20-25 times). To standardize the throw counts for distances when ranges were given, the median throw of the range was used (i.e. range was 20-25, 23 throws was used in the code).
For the mound progression, the throws were prescribed with various intensities (e.g. 15 throws at 50%). Previous research has shown that asking pitchers to throw at decreased intensity, there was not a proportionate decrease in ball velocity or elbow varus torque.15,27 Therefore, we used Dowling et al’s9 linear regression model of prescribed intensity and resulting torque.
Stage 3 of the original ITP allowed for players to start pitching breaking ball pitches. These were instructed to throw with decreased intensity compared to the fastball pitches. Biomechanical studies have shown that resultant loads in the throwing arm are similar for the fastball and curveball in pitchers.24–26 Thus, pitch types were not differentiated and fastball elbow varus torque was used for the workload calculations. However, we delineated between intensity when identified in the original program.
RESULTS
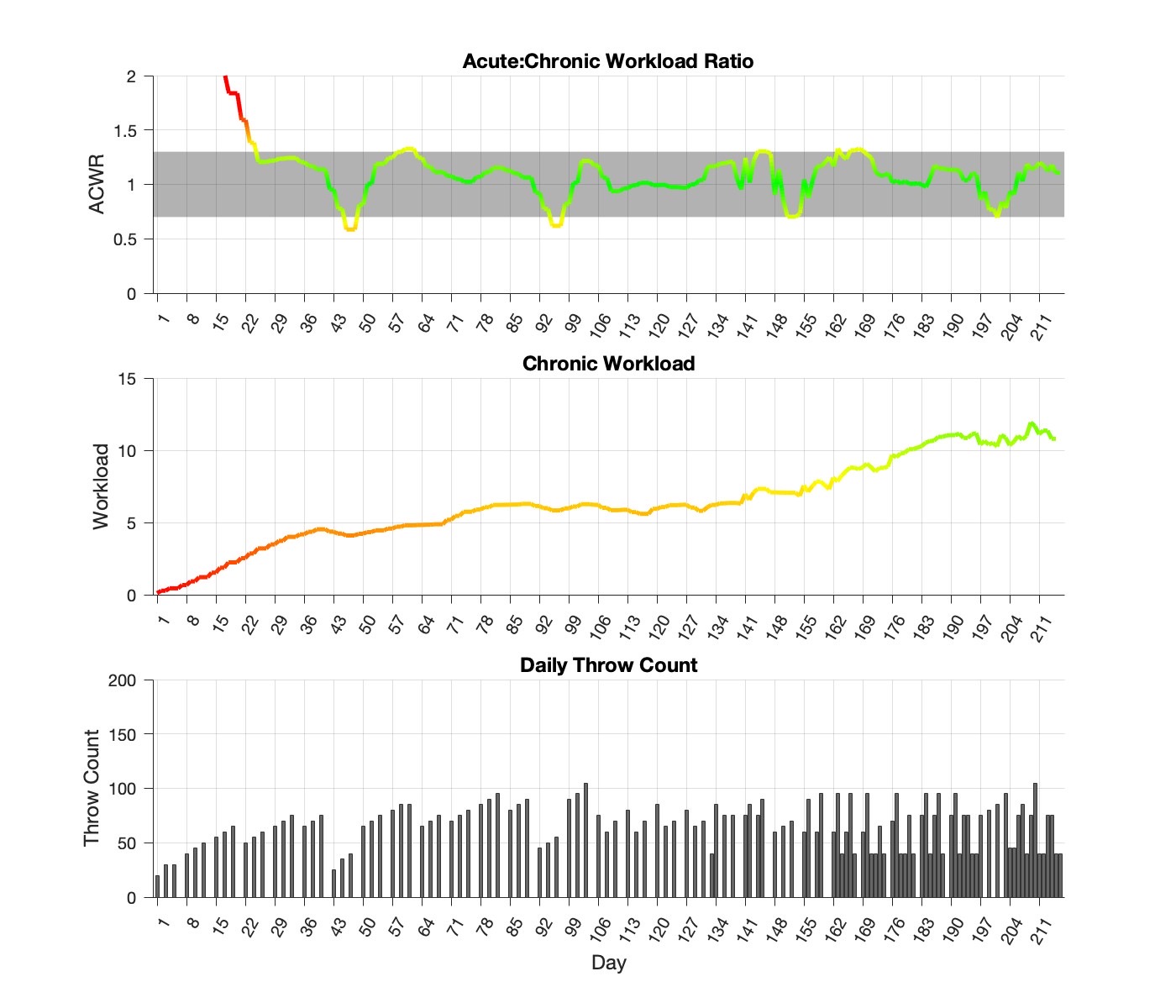
The updated program was comprised of a 217-day schedule (Figure 2). The flat-ground progression was a total of 105 days with 45 of them being throwing days. The mound progression consisted of 112 days with 75 of them were throwing days. The program finished with a chronic workload of 10.8. After the initial 28 days, the updated program’s ACWR exceeded 1.3 eleven times, and below 0.7 seven times. ACWR stayed within the safe range (0.7 - 1.3) for 91% of the program, peaking at 1.33, or 2% over the desired range.

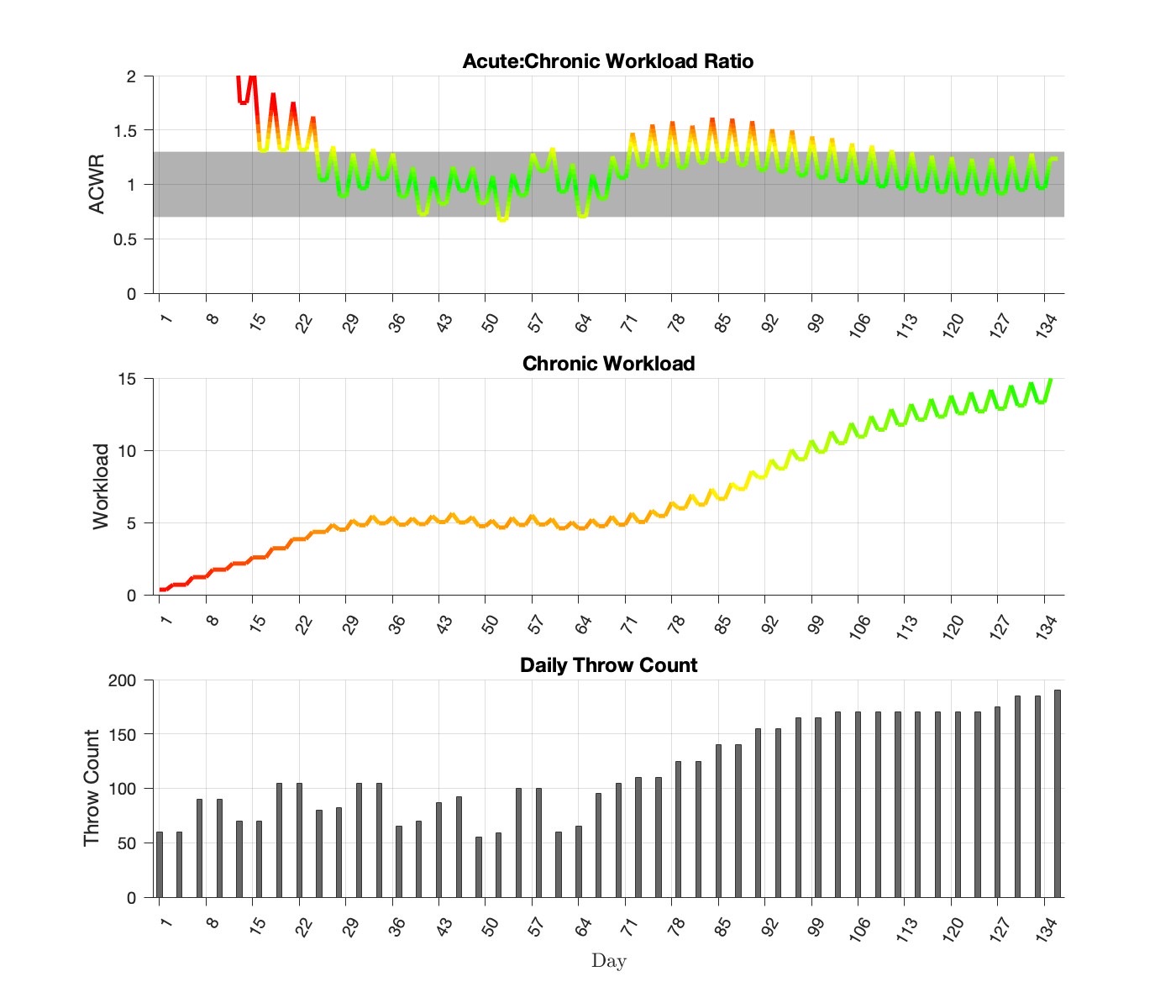
The original program consisted of a 136-day throwing schedule with the first 72 days in the flat-ground progression and 64 days in the mound progression (Figure 3). Actual days throwing were 24 and 22 for the flat-ground and mound progressions, respectively. The original program finished with a chronic workload of 15.0. During the original program, the ACWR deviated above the safe-threshold of 0.7-1.3, two and seventeen times, respectively. ACWR fell within the safe range for 82% of the program and peaked at 1.61, or 24% higher than the desired range.

DISCUSSION
The original ITP developed by Reinold et al10 has been utilized for decades without significant updates to the program. This program was designed based on the clinical experience of the authors and with limited biomechanical evidence. However, our understanding of the biomechanics of ITPs and workload implications have evolved significantly since its publication. Anecdotally, traditional ITPs have come under recent criticism by baseball coaches and players as not meeting the needs of the modern baseball pitcher. Therefore, an updated program was designed that considers a modern approach to baseball throwing programs. This ITP was designed to represent a modern throwing program that is commonly performed and familiar to baseball pitchers. It eliminates some of the variables of the original program such as sets and repetitions of throws, breaks during a throwing session, and repeating steps several times without progressing.
The updated ITP did an excellent job at progressing chronic workload and ACWR. This program builds to a final chronic workload of 10.8 over a 7-month period. In comparison to the original program, that finished with a final chronic workload of 15.0 in a much shorter amount of time. This longer and more gradual progression in the updated ITP may be beneficial to the healing tissues and may be more tolerable as modern pitchers are throwing with higher velocity and load to the arm.
In a study on baseball pitching workloads, Mehta et al28 reported that higher chronic workloads were associated with an increased risk of injury. In-season chronic workloads have been observed to be between 12-15 in high school,28 as well as in college and professional baseball pitchers (Motus Global unpublished). Since the purpose of the ITP is to return an injured pitcher back to competition, the chronic workload at the conclusion of the ITP should approach, not meet, the maximum chronic workloads observed during a normal season. Rather, it should allow room to increase as the pitcher finishes their rehab assignment (i.e. throwing live at-bats, simulated games, incrementing innings, etc.) and returns to full competition. This would allow workload to continue to build within a normal range over the course of the subsequent competitive season and not exceed commonly observed chronic workload levels. The original ITP reached a chronic workload level equivalent to midseason workload levels by the end of the ITP. Anecdotally, this may be why it is common for pitchers to return following surgery with reports of fatigue and decreased velocity the first year back, and then a return to normal or improvement in year two.29,30
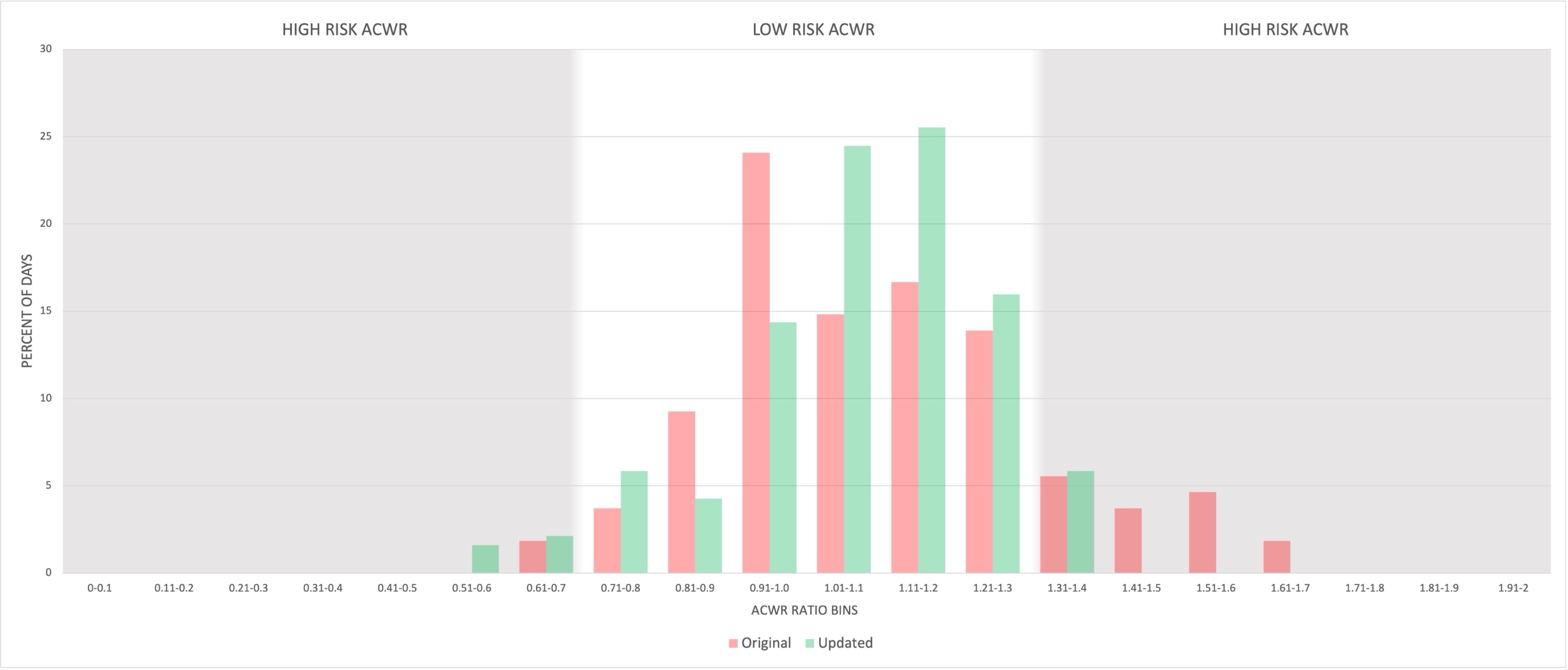
There has been a reported correlation between increased ACWR and injury risk.19–23 Mehta23 reported in a cohort of 18 high school pitchers that a greater chance of throwing-related injuries occurred in pitchers whose ACWR exceed 1.27. Pitchers whose workload exceeded this ACWR exhibited a 15 times increased chance of injury compared to pitchers below this ACWR threshold. ACWR during the updated ITP was shown to fall within the desired range of 0.7 and 1.3 more often than the original ITP. The original program was in the desired range for 82% of the program in comparison to 91% for the updated program. Furthermore, the peak workloads in the original program were higher, up to 1.61 ACWR or 24% higher, for approximately 10% of the program, The updated program that just barely dips below and rises above the desired range (Figure 4). This may result in a more tolerable progression for athletes and avoid periods of excessive fatigue, discomfort or even setbacks all while increasing capacity and readiness.

Both the original and updated ITP programs begin with a high ACWR in the first 28 days because there is no chronic workload in the days preceding the program. Both ITPs assume that the pitcher has not thrown during rehabilitation and would be starting with a chronic workload of 0. However, recent shifts in rehabilitation have emphasized pitchers using the throwing motion drills prior, such as towel drills, sock drills, and 1-arm plyometrics, to initiating a formal ITP, which theoretically could build workload. Rehabilitation protocols have emphasized using plyometric exercises before the pitcher is allowed to start throwing which could build workload as well.31,32 Additionally, the load on the throwing arm at such short distances at the beginning of the ITP is so low that we do not feel this high ACWR initially is clinically concerning.
Distance was used as the variable to progress flat-ground intensity and load to the throwing arm. Some authors have recently suggested the use of radar guns to monitor intensity during ITP as they are unable to adequately match effort and actual throwing arm load.33 However, studies have shown that throwing velocity does not correlate with elbow torque and varies per pitcher,34–36 making the use of a radar gun less accurate for an ITP. Coaches and clinicians use a radar gun to help determine and regulate a pitcher’s effort, but many experts agree that using a radar gun shifts the emphasis to velocity of a throw rather than focusing on proper mechanics.8 The correlation between distance and torque is shown in Figure 1, and allows a more reliable and gradual progression in stress than using velocity.
In regards to perceived effort of throwing off the mound, it is known that perceived intensity does not correlate to throwing velocity or elbow varus torque. Pitching at 50% effort corresponds to 80%-85% of maximum ball velocity and 75% of maximum elbow varus torque.15,27 Pitching with 75% effort corresponds to 85%-90% ball velocity and about 80% - 90% elbow varus torque.15,27 The relationship between percent effort and elbow torque was built into our throwing workload model.
The updated ITP was designed for long-term rehabilitation programs for shoulder and elbow injuries. The authors recommend that this ITP typically begin 20 weeks after most surgical procedures, such as Tommy John reconstruction. However, many factors can influence the beginning of an ITP such as the surgery performed, pitcher’s age, level of competition, time of season, surgeon’s preference, and successful progression through the rehabilitation process. Because the updated program is 217 days, if a pitcher starts 20 weeks after surgery, successful completion and to return to competition would be around the 12-month mark after surgery. However, after the pitcher finishes the ITP there is still a gradual build-up of live at-bats, simulated games, and full-intensity innings before the pitcher is allowed to 100% return to competition.
It should be noted that long toss past 120 feet and weighted ball programs were intentionally not included in this updated rehabilitation ITP. Both have been shown to potentially produce more load to the throwing arm than pitching a regulation ball off a mound, making it difficult to control the gradual workload buildup.15,37–40 All ITPs are designed to gradually increase throwing arm load to effectively prepare a pitcher for stress involved with competitive pitching. As the player transitions to the competitive season, the inclusion of extreme long toss and weighted balls can be individualized for each pitcher. The risks and rewards of extreme long-toss and weighted balls in performance and maintenance programs for active pitchers are beyond the scope of this study investigating rehabilitation throwing programs.
The updated ITP detailed the inclusion of deload weeks at four different points, spaced out during the program. The concept of deloading has been popularized in strength and conditioning and theorized to allow the body a brief period of recovery when going through a long duration of linear loading. Anecdotally, pitchers often report periods of fatigue and generalized soreness over the course of the ITP. The deload period allows the body to recover before continuing to the next, and often with increased intensity, phases of the program. The inclusion of deload weeks in the updated ITP required a strategic plan when returning to the throwing progression to assure appropriate ACWR was maintained. The inclusion of the deload weeks arguably had a negative effect on the buildup of chronic workload and drop in ACWR below the safe range of 0.7. We believe the benefit of giving the athlete a physical and mental break from the long rehabilitation process is ultimately more advantageous in the long run, as long as the ACWR is accounted for appropriately after the deload period.
There are a few limitations to the current study that should be mentioned. The data used to analyze the ITP workloads was determined using data for healthy high school and collegiate pitchers reported by Melugin et al27 and Dowling et al.9 The relationships between elbow torque and workload with types of throws may vary for pitchers of different age, height, weight, and throwing mechanics. The individual needs of each player must always be addressed when designing any ITP. The optimal ITP may vary for different pitching injuries. Our computational model of throwing workload was predicated on biomechanical studies of elbow varus torque and may therefore be most applicable to pitchers recovering from surgical treatment of UCL injuries. Variations of this program should be designed that take into consideration shorter or longer durations based on the specific athlete and injury.
CONCLUSION
We have introduced an updated ITP based upon our current understanding of the biomechanics of throwing programs and built to represent the needs of the modern baseball pitcher. The proposed ITP has a more gradual and consistent workload progression than past ITPs, as measure by chronic workload and ACWR. This program can be used to return pitchers back to baseball pitching during long-term rehabilitation programs for shoulder and elbow injuries.