

INTRODUCTION
Skilled post-operative rehabilitation after anterior cruciate ligament reconstruction (ACLR) with a specific focus on quadriceps strength symmetry has been a topic of increased attention especially in athletes returning to a pivoting sport.1–4 A variety of return-to-sport (RTS) assessments and protocols have been suggested with evidence suggesting a decreased risk of reinjury based on passing certain criteria including quadriceps strength symmetry.2,5 Limb symmetry index (LSI) testing has become one of the most common ways to assess strength between limbs to help the patient and clinician customize exercise progressions.1,4,5 Pre-operatively and post-operatively, one of the more common inquiries patients have is when they would be estimated to reach certain quadriceps strength milestones to allow them to progress to activities like running and other activities.
The purpose of this study was to evaluate the range of quadriceps strength percentage and function benchmarks at various points after anterior cruciate ligament reconstruction surgery based on sex, age, and graft. The hypothesis was that most patients, especially autograft ACL reconstructions, will not reach 80% quadriceps symmetry until 4-6 months post-operatively.
METHODS
After institutional review board approval, a REDCap database was established to collect demographic and outcomes data. Patients who underwent ACLR were evaluated at various points after surgery by one of the author team physical therapists and informed consent was obtained from the patient. Rights of the patient were protected. Surgeries were performed by various surgeons with unknown surgical technique other than type of graft utilized.
A handheld dynamometer (HHD) (MicroFET2 - Hoggan Scientific, Salt Lake City, Utah) was stabilized against an open-chain knee extension machine arm that was locked in a fixed position at 60 degrees of flexion (Figure 1).

This fixed position provides a more universal medium for strength examination and reduces the dependency on the measurer. Examiners included four experienced sports physical therapists who used the same setup and HHD device. All patients performed maximum effort knee extension against the HHD for three trials of five-second contractions and the average of these trials was recorded. Timing of this testing varied by patient physical comfort and ability to perform single leg strength training exercises such as step-downs, split squats, and single-leg dead lift without significant pain. This usually started 8-12 weeks form surgery. Clearance to initiate a walk-to-run progression was initiated when the patient had minimal to no effusion on physical exam (Sweep test), had no pain with loading the knee with walking/light impact, stationary hop mechanics showed adequate load absorption (judged by physical therapist), and when the quadriceps index was at least 80%. Clearance to full activity and agility sport (if applicable) was when the patient underwent a standardized functional movement assessment (FMA) and the patient exhibited no pain, no effusion, quadriceps index over 90%, tolerated jogging, and hop testing (single leg, triple leg, crossover hop) was greater than 90% compared to the uninvolved limb, with good mechanics (as judged by the physical therapist: including no significant dynamic knee valgus or hip drop, appropriate knee excursion, and able to stick landing without loss of balance, etc). The same series of tests was used by all physical therapists and patients.
Descriptive statistics including mean and standard deviation for continuous variables and frequency and proportion for categorical variables were calculated to characterize the study group. The progression of quadriceps symmetry throughout the postoperative period was examined with multi-level models. A varying intercept at the patient level was included to account for repeated observations along with a varying slope for postoperative months to allow the effect of time on symmetry to vary across patients. Estimates of time to reach 70%, 80%, and 90% quadriceps symmetry were obtained from the fitted model, which included fixed effects for graft and sex. To explore the role of age, the model was extended to include patients of age less than 25 and patients 25 or greater. Results of inferential analyses are presented with 95% confidence intervals. All analyses with performed using R version 4.2.1 (R Core Team 2022) and the following packages: lme46 and ggeffects.6
RESULTS
A total of 164 patients were evaluated (98 female, 66 male) who underwent ACL reconstruction. Patients either received bone-tendon-bone (BTB) autograft (n=118) or BTB allograft (n=46) for their ACL graft. Average age was 31.1 years-of-age (SD: 13.6). The multilevel model for progression of quadriceps symmetry over postoperative period is presented in Table 1.
The estimated time to reach quadriceps symmetry thresholds were evaluated by sex and graft type (Table 2, Figure 1).
A group of age under 25 years was added to the model to better reflect high school and collegiate athletes (Table 3).
On average, patients undergoing ACLR using BTB autograft (n=65) were estimated to achieve 70% quad symmetry at an average of 4.1 months, 80% at 7.1 months, and 90% at 10.2 months. Females were cleared to run at an average of 6.8 months and were able to pass a FMA exam at an average of 10 months. On average, males undergoing ACLR using BTB autograft (n=53) were estimated to achieve 70% quad symmetry at an average of 2.6 months, 80% at 5.7 months, and 90% at 8.7 months. Males were cleared to run at an average of 5.6 months and were able to pass a FMA exam at an average of 8.5 months.
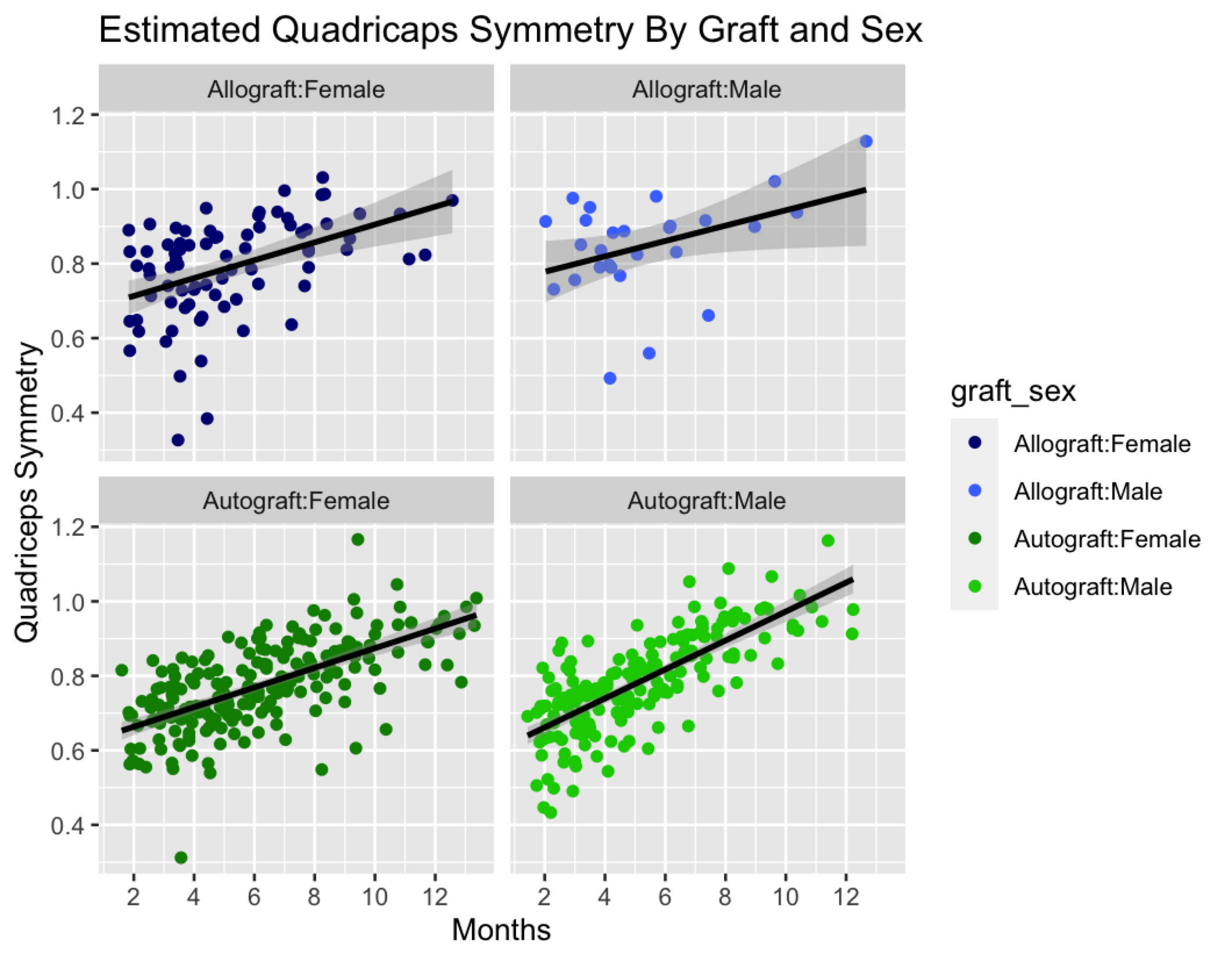
Patients undergoing ACL allograft were evaluated and separated by sex. On average, females undergoing ACLR using allograft (n=33, mean age 48.7 +/-7.0) were estimated to achieve 70% quad symmetry at an average of 2.3 months, 80% at 5.4 months, and 90% at 8.4 months. Average time to be cleared to return to running for female allografts was 5.8 months. Only two of 33 (6%) female patients were able to pass a FMA exam at an average of 8.3 months. On average, males undergoing ACLR using allograft (n=13, mean age 50.9 +/- 8.1) were estimated to achieve 70% quad symmetry at an average of 0.9 months, 80% at 3.9 months, and 90% at 7.0 months. Average time to be cleared for running for male allografts was 4.5 months (+/-2.0 months). Only 1 of 13 (8%) male patients passed an FMA exam at an average of 6.2 months.
Females under the age of 25 years-of-age (n=48, mean age 18.8 +/- 2.7) undergoing ACLR using BTB autograft were estimated to achieve 70% quad symmetry at an average of 3.91 months, 80% at 6.96 months, and 90% at 10.0 months. Average clearance to return to running was 4.7 months (+/-2.7) and clearance to full activities 9.0 months (+/- 1.7). Males under the age of 25 years-of-age (n=29, mean age 21.0 +/- 3.1) undergoing ACLR using BTB autograft were estimated to achieve 70% quad symmetry at an average of 2.40 months, 80% at 5.44 months, and 90% at 8.49 months. Average clearance to return to running was 3.3 months (+/-1.8) and clearance to full activities 6.6 months (+/- 2.6). Tables 3 and 4 further illustrates this breakdown by age.
Table 5 further evaluates the probability of patient testing out with various quadriceps percentages at different points after surgery based on confidence intervals.
DISCUSSION
The rehabilitation of ACL surgery is a widely discussed clinical phenomena with a myriad of methods and reviews articles available.7–9 One of the most important factors that makes a clinical difference not only on patient reported outcomes but also ACL re-injury rates is quadriceps strength.10–12 With only 55-80% of athletes reported to return to competitive sports there is opportunity for providers to optimize the recovery of patients with the goal of increasing the percentage of athletes that return to their pre-injury level of competition.13–15 Recognition of the importance of quadriceps strength symmetry can help decrease complications in athletes at the time of their return to sport and create a more accurate guideline for patients and providers to refer to during their recovery period rather than chronological guidelnes.2,5
The results of this study demonstrate a slower estimated progression of quadriceps strength return in patients who underwent BTB autografts in comparison to BTB allograft procedures regardless of age or sex. It took both males and females under 25 who underwent a BTB autograft over two months longer on average to reach the same quadriceps milestones (70%, 80%, 90%) as those who underwent allografts. This result is expected due to the increased trauma the knee experiences during graft harvest in patients undergoing reconstruction using autografts. While a difference was observed between the estimated average recovery time for males and females, the difference in average time was not significantly different. Hannon et al. stated that age and sex only added 0.8% of variance for quad strength which is supported by the results of the current investigation.16 In counseling patients (and parents of younger patients), describing evidence-based expectations are important to establish especially given the notably high risk of re-injury (including contralateral injury) or ACL re-tear in the under-20 years-of-age population.17–20
Limitations
Limitations of this study include that only a small patient population that underwent allograft procedures. With only 13 males over 25 undergoing allograft reconstructions, the results may not be entirely representative of the recovery timeline for the larger population. Another limitation includes the separation of patients into cohorts based on age to represent athletic status may similarly misrepresent the larger population. A total of only three patients out of a possible 46 allograft patients passed an FMA exam though all 46 attempted testing. It is unclear if patients simply elected to discontinue PT before passing it having achieved their relative goals or if they simply could not pass this in general. In order to fully account for outliers in overall quadriceps strength, future studies could separate patients based on pre-surgical quadriceps strength instead of age. Strengths of this study include the objective assessment of muscle strength and evaluation of hop mechanics by four experienced sports medicine physical therapists via the same methodologies.
CONCLUSION
Patients undergoing BTB autograft are estimated to obtain 80% quadriceps symmetry at an average of 5.7 months for males and 7.1 months for females. Individuals under the age of 25 obtain their quadriceps symmetry faster and are cleared to return to running faster than individuals over 25. Male sex is associated with decreased amount of time to obtain clearance for running and for full activity. Male sex is associated with a decreased amount of time to regain quadriceps symmetry however this was not significant.