

INTRODUCTION
Shoulder injury and pain are among the most prevalent musculoskeletal complaints, ranking third in reporting to primary care1 and a lifetime prevalence of 67%.2 Daily shoulder pain has been reported within 30% of the working population,3 with chronic shoulder pain occurring in approximately 50% of all cases.2 However, pain and injury prevalence has been reported to be much higher in overhead sports. Research has shown shoulder pain history in 44-75% of elite handball players,4 with injury occurrence recorded at 48% in tennis,5 23% in cricket6 and 31% in baseball.7 Shoulder injury occurrence in overhead athletes is usually as a result of breakdown(s) in the function of the upper extremity kinetic chain (KC) which causes mechanical adaptations and performance dysfunction.8 Injuries and adaptations have been reported to include acquired glenohumeral instability, Glenohumeral Internal Rotation Deficit (GIRD), scapular muscle imbalances, scapular dyskinesis, and rotator cuff disease.9–12
In order to assess diagnosis and management strategies in populations with shoulder injury, understanding of functional performance, impact on quality of life through measures of health and well-being, and greater appreciation of the ramifications of pain are required.13 Functional assessment of the shoulder can be categorized as either a self-report measure (SRM) or a physical performance measure (PPM),14 although little focus has been given to identifying similarities and differences between healthy and injured overhead athletes during functional movement. Several testing protocols are available to practitioners to assess the function of the injured limb, with the vast majority focusing on requiring the injured patient to complete an everyday movement or task. The Simple Shoulder Endurance Test,15 involves turning and twisting bolts but in a single position and although this is an endurance-based test, it does not consider the broader functional demands of the shoulder. The most recently published testing protocol is the Timed Functional Arm and Shoulder Test (TFAST),16 consisting of three main tasks, each assessing the endurance, ROM and strength of the injured shoulder and focused on reaching, circular upper extremity motion, and lifting related tasks. Another performance-based test of upper extremity function is the 9-Hole Peg Test, whereby patients pick up pegs and place them into specified holes.17
One of the most popular testing protocols for functionality is the FIT-HaNSA (Functional Impairment Test-Hand and Neck/Shoulder/Arm) which is a functional assessment designed to test the upper extremity across multiple levels with the aim of simulating daily activities.18 The protocol consists of a test battery of three tasks, each lasting up to five minutes or until the participant feels unable to continue any longer. The three tasks consisted of a “waist-up” movement, an “eyedown” movement and an “overhead work” movement. Kumta and colleagues19 correlated FIT-HaNSA scores with shoulder strength measurements and found positive correlations for flexion (r = 0.66) and abduction (r = 0.55). Research on symptomatic patients using the FIT-HaNSA protocol has produced important findings; firstly, patients with impingement had issues completing the “eye-down” task, averaging a total task performance time of 246s out of a maximum of 300s18; and secondly, when comparing healthy controls to a symptomatic group with sub-acromial impingement syndrome (SAIS) the latter group scored significantly lower overall (59.9% vs. 98.5%) as well as on each individual task.13 FIT-HaNSA has also been used to assess functionality in patients with a massive rotator cuff tears and were found to have increased rotator cuff and latissimus dorsi (LD) activity during the elevation phase of the “waist-up” protocol.20 This was attributed to the increased need to provide stability of the glenohumeral (GH) joint. Due to this being the only protocol with previously published muscle activity findings, although for only one movement, it may be the most effective protocol to assess muscle activities across different types of performers as it requires a controlled environment and relies little on skill to complete.
While previous research studies have focussed on functional movements in injured populations,18,20 several more-recent studies have investigated the impact of fatigue in overhead athletes,21–23 during movement assessment of athletes with and without shoulder injury24 and preventative/ rehabilitative exercises.25–28 However, there is a lack of information relating to utilising functional tests to assess muscle activity during controlled, non-skilled everyday tasks. As a result, this study aimed to identify muscle activities across fourteen upper extremity and core muscles during three functional everyday movements in athletes with and without history of shoulder injury.
METHODS
Participants
A total of thirty-two male overhead throwing athletes participated in this study; fifteen were healthy (age: 25.1 ± 6.7 years) and seventeen were injured (age: 32.7 ± 10.7 years). All participants were overhead athletes recruited from local and regional baseball, cricket and handball sports clubs, and were allocated into two groups; healthy and injured. Inclusion criteria was based on shoulder injury history, with healthy defined as those who had no history of injury to their throwing shoulder or upper limb. Injured participants had a clinical history of shoulder injury (i.e. shoulder instability [n = 3] or rotator cuff disease [n = 14]) within the previous three years, as well as difficulty or pain during performance indicated in the Sports Module section of the quick Disability of the Arm, Shoulder and Hand (qDASH) questionnaire. Overhead athletes were excluded if they had no history of shoulder injury but registered difficulty or pain when completing the qDASH. The study received ethical approval from the national Research Ethics Committee. All participants were provided with a detailed information sheet at least 72 hours before their participation outlining the main details of the project and measurement procedures. All participants gave written consent before undertaking any data collection.
Functional Tasks
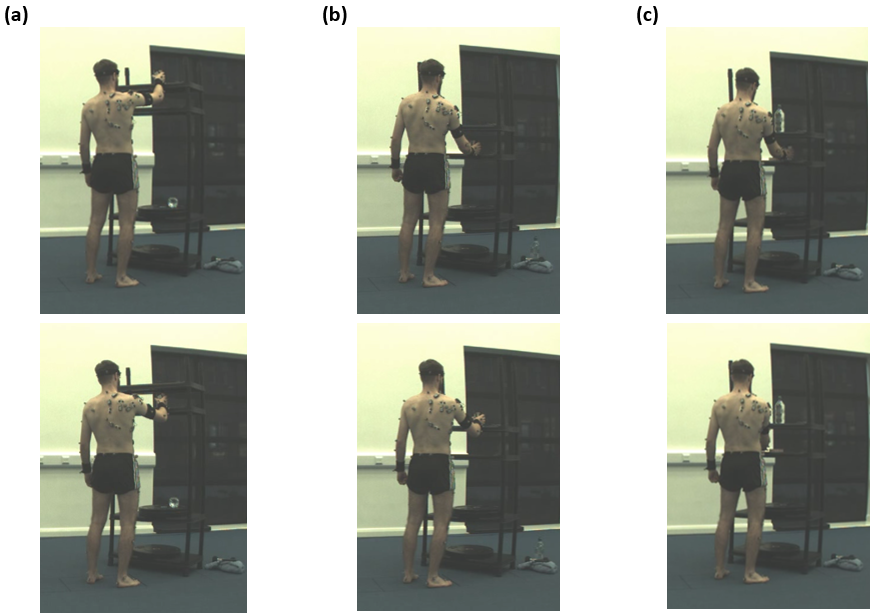
Three everyday functional movements using the dominant arm (high elevation, low elevation and rotation) were investigated (Figure 1). The high and low elevation tasks were adapted from the FIT-HaNSA protocol18 which requires participants to move a tin can (1kg) between two fixed positions at 25cm height increments. For the rotation task, participants moved the tin can between two fixed positions, 20cm apart, on a shelf positioned at waist height. Each movement was divided into two phases for data analysis purposes. For high elevation, Phase 1 was defined as the tin can moving from the top shelf to the bottom shelf and Phase 2 defined as bottom to top. For low elevation, Phase 1 was defined as the tin can moving from bottom shelf to top shelf and Phase 2 defined from top to bottom. For the rotation task, Phase 1 was defined as the tin can being moved medially across the shelf and the arm internally rotating and Phase 2 defined as the tin can being moved laterally across the shelf and the arm externally rotating.
_high_elevation_(b)_low_elevation_(c)_rotation.png)
Measurement Protocol
A 16-channel TeleMyo TDS System (Noraxon USA, Inc., Scottsdale, Arizona, USA) and associated MyoResearch software (version 3.8.6) were used for signal acquisition, processing, and analysis. Raw EMG signals were amplified (CMR: > 100 dB; input impedance: > 100 Mohm; and Base Gain: 200 dB), with signals collected at 1500 Hz and band-pass filtered at 20 to 250 Hz for surface electrodes and at 20 to 350 Hz for fine-wire electrodes.
Self-adhesive Ag/AgCL snap, surface dual electrodes (Noraxon USA, Inc) were placed parallel with the muscle fibers, with an inter-electrode distance of 20mm, to record EMG from muscles across KC segments. Surface EMG was collected for thirteen muscles; biceps brachii (BB), anterior, medial and posterior deltoids (AD, MD, PD), upper and lower trapezius (UT and LT), pectoralis major (PM), latissimus dorsi (LD), serratus anterior (SA), infraspinatus (ISP), contralateral and ipsilateral external bliques (contraEO and ipsilEO), and gluteus maximus (GM). Skin preparation included shaving the site and cleaning by an alcohol-free moist tissue (Kay’s Medical, UK). Fine-wire electrodes were used to record signals from the supraspinatus (SSP) using a disposable bi-polar hook intramuscular fine-wire electrode (size: 0.50x30mm (10cm wire)) (Spes Medica S.r.l., Genova, Italy) using a hypodermic needle.29
Raw EMG signals from twelve full cycles for each task (the first two and last two cycles omitted for consistency purposes) were smoothed (1500 sample/window), full-wave rectified (400 sample/window) and a root mean square (RMS) amplitude algorithm with a window size of 100ms applied. EMG from each muscle was recorded during Maximal Voluntary Contraction (MVC) for normalisation purposes. Manual muscle testing was performed by the lead investigator using procedures previously reported in functional exercise research.30–34 Two, five second efforts, with verbal encouragement, were recorded for each muscle, with the mean calculated for normalization during each functional task and reported as %MVC. A one-minute rest period was permitted between each MVC trial.
Data Analysis
Descriptive statistics are reported as %MVC for each individual muscle (mean ± standard deviation [SD]) during each phase of functional everyday task. Mixed model repeated measures ANOVA tests were performed for each functional task to determine group effects, time (phase) effects and interaction between them. Mauchly’s Test of Sphericity was performed to assess the variance of within-subject conditions35 and on occurrences of violation (p < 0.05), the appropriate epsilon correction was chosen (> 0.75, a Huynh-Feldt correction was applied; < 0.75, a Greenhouse-Geisser correction was applied). Post-hoc independent t-tests were performed to assess the statistical differences between groups during each phase of each functional task for mean activity values. The level of statistical significance was set at p < 0.05. SPSS (Statistical Package for Social Sciences, version 25) was used for all data analysis procedures.
RESULTS
Table 1 summarizes the mean activation of muscles during each functional task.
High Elevation
Significant time effects were evident for PM (p = 0.000), LD (p = 0.003), all deltoid (AD: p = 0.000; MD: p = 0.041; PD: p = 0.000), trapezius (UT: p = 0.000; LT: p = 0.000) and rotator cuff musculature (SSP: p = 0.024; ISP: p = 0.000). However, post-hoc tests found no differences in mean activity between groups during downward (Phase 1) or upward (Phase 2) movements.

Low Elevation
Significant time effects were evident for BB (p = 0.001), trapezius muscles (UT: p = 0.001; LT: p = 0.002), ISP (p = 0.000) and GM (p = 0.049). Post-hoc tests determined no differences in mean activity between groups upward (Phase 1) or downward (Phase 2) movements.

Rotation
A significant group effect was evident for UT (p = 0.038) only. Significant time effects were evident for the AD (p = 0.033 and PM (p = 0.034). Post-hoc tests revealed significant differences in mean UT activity between groups during both medial movement (Phase 1: p = 0.038) and lateral movement (p = 0.048). In both phases, mean UT activity was higher in healthy overhead athletes compared to injured (Phase 1: 6.0 %MVC (± 5.3) compared to 2.7 %MVC (± 2.1); Phase 2: 6.1 %MVC (± 5.1) compared to 3.0 %MVC (± 2.5)).

DISCUSSION
This research study investigated differences in muscle activities of fourteen muscles across upper extremity and core segments during three everyday tasks in overhead athletes with and without shoulder injury. Across elevation and rotational functional tasks, only significant differences in mean UT activity during both phases of the rotational task were evident, with greater UT activity recorded in healthy overhead athletes. However, potential compensatory mechanisms between key scapula and rotator cuff muscles may be evident in injured throwers to assist in humeral elevation and internal rotation of the arm.
In addition to the higher mean UT activity, differences in UT activity patterns were also evident throughout the rotational functional task movement cycle, with three distinct peaks identified for healthy overhead athletes that were not evident in injured overhead athletes (Figure 4). The healthy group appear to activate the UT to assist with raising the tin can, most notably around as the arm internally rotates over mid-shelf during Phase 1 and again at the start of Phase 2 as the tin can was lifted back off the shelf at the start of the external rotation phase. In addition, UT activity increases for a third time as the arm is lowered back to the start point. Actions of the UT encompass both scapular control and clavicle elevation36 and the activity profiles identified in this research study could be a method employed by the healthy group to assist in glenohumeral joint stability but also in elevating the clavicle to assist in clearance and initial elevation. In contrast, injured throwers elicited more SSP activity when lifting the tin can off the shelf and internally rotating across mid-shelf. This suggests SSP activity is needed during humeral elevation as previously proposed by Otis and colleagues37 and to counteract the reduction in UT activity at these points of the movement cycle which may increase the risk of impingement.
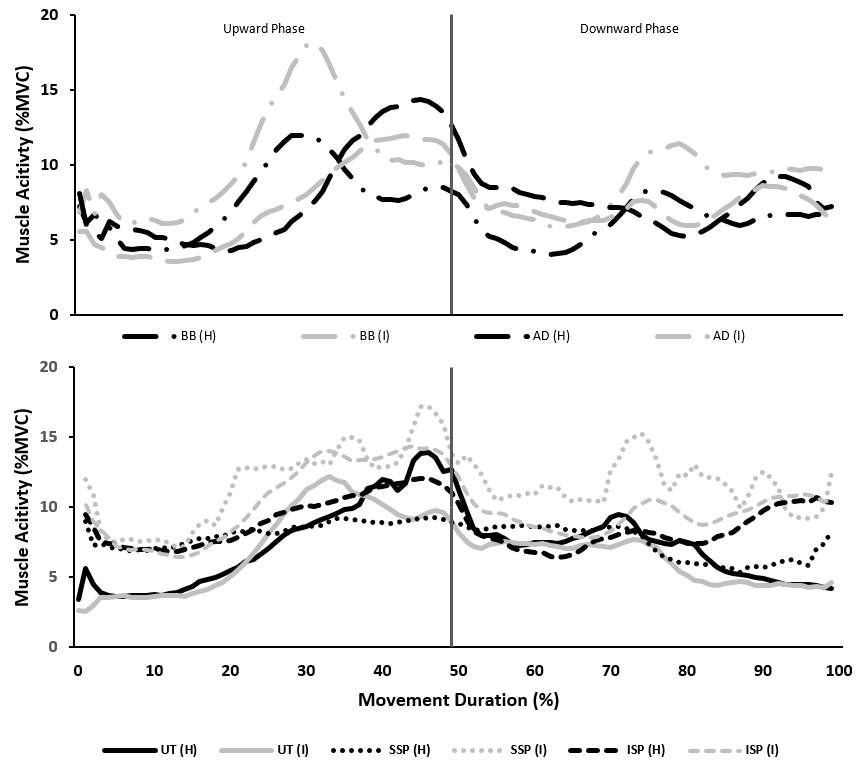
The High Elevation protocol required participants to move a tin can from a shelf positioned at eye level to another 25cm below before returning it to the higher shelf. The findings of this study identified no differences between healthy and injured groups for mean muscle activation either during or between phases for this protocol, although differences in muscle activity patterns were evident. Activity patterns for the AD, UT and rotator cuff musculature exhibited some variation between healthy and injured throwers, agreeing with findings in previous research studies investigating shoulder elevation tasks.13,38 At mid-elevation, AD and UT activity increased as rotator cuff activity increased, with higher SSP and ISP activity evident in injured throwers (Figure 2). This supports the previous findings of Hawkes and colleagues,20 who attributed increased rotator cuff activity as a mechanism to ensure glenohumeral joint stability during arm elevation movements. In addition, patients with anterior shoulder instability exhibited higher peak ISP, UT and PD activity, but lower SSP activity when compared to healthy controls during elevation tasks.38 They deemed activity differences were significant around mid-elevation and determined that the early onset of ISP and SSP resulted in delayed onset of UT activity. This is in slight contrast to the findings of the present study, as although ISP and SSP activity were higher in injured throwers during mid-elevation, UT activity was lower when compared to healthy throwers. This suggests that injured throwers utilize rotator cuff musculature to compensate for reduced UT activity as the arm is elevated. During the mid-elevation range through to the end of Phase 2 as the arm is raised to its highest point, healthy throwers exhibited higher AD, UT and LT activity whereas injured throwers exhibited higher ISP, SSP, MD and PD activity. The increased eccentric activities of both the SSP and PD could be strategies to counteract AD activity as it contracts to flex the shoulder joint and in turn, aid repositioning of the humeral head during upward movement39 to support humeral elevation37 similar to the previously proposed mechanism during the rotation task.
Similar to the High Elevation protocol, no mean muscle activity differences were evident between groups during or between phases for the Low Elevation protocol. However, differences in activity patterns were evident around mid-elevation in both upward and downward phases for the same muscles as previously highlighted. Therefore, it is suggested that similar compensatory mechanisms should be applied towards this protocol. However, differences in BB activity patterns were noted for this protocol. The BB plays an important role during initial arm elevation, and when the arm is elevated to 30o, the BB provides stability to the glenohumeral joint as it moves through the range.40 In the present study, BB activity increased in both groups approaching mid-elevation during the upward phase, although activity was higher in injured throwers. This activity could be as a result of increased elbow flexion mid-elevation, although it is possible that the higher BB activity exhibited in injured throwers was required to assist in providing additional stability to the shoulder joint during the upward movement. Landin and colleagues41 reported that continued BB activity was evident when the arm was further elevated past 30o and this activity is in combination with increased AD activity as the shoulder continues to be flexed.42 This is consistent with the findings of the present study, with peak AD activity being exhibited in both groups after peak BB activity, approaching the end of the upward phase (Figure 3). Healthy throwers also exhibited a greater peak activity of AD compared to BB which contrasts the activity magnitudes of injured throwers. Peak BB activity during the downward phase was less than peak activity during the upward phase for both groups. This could suggest that muscle activity needs to be increased in the upward phase due to working against gravity (as proposed by Hawkes and colleagues),20 but also as a result of the need to enhance glenohumeral joint stability and reduce the anterior translation of the humeral head.43 BB activity patterns identified in this present study are comparable to those previously reported in similar studies,20 which detailed a gradual reduction in BB activity until around 70% of the movement cycle, where re-activation is evident.
Future studies should focus attention towards increasing the weight of the object being manipulated during functional everyday tasks, or increase the time permitted to complete the task. The fatiguability of key muscles could be investigated alongside postural movement during each trial. Due to the ballistic movement associated with overhead throwing, functional movements at greater speeds could be investigated to assess muscle activities across the upper extremity and core, and identify differences between healthy and injured throwers. This may provide further insights to those provided by Castillo-Lozano and colleagues44 who investigated the muscle activity of healthy participants during arm elevation through different planes and at different speeds. This may provide an intermediate test condition between controlled functional and throwing-related movements. Finally, for overhead throwing athletes, more complex functional tasks could be designed that reflect similar movements to an overhead throwing task where participants move through various planes of movement in succession.
CONCLUSION
The results of this study present the activity of selected upper extremity and core muscle in healthy and injured overhead throwing athletes during three functional everyday tasks (high elevation, low elevation, and rotation). While both groups recorded similar mean activities for high and low elevation movements, healthy throwers elicited higher UT activity during both phases of the rotational movement. Qualitative examination of muscle activity patterns presented temporal shifts in muscle activation timings and magnitudes which could relate to potential compensatory mechanisms in order to achieve task completion.
The functional movements were designed to allow the participants to complete tasks without any inhibitory or adaptations in technique, controlling the intensity of action demanded on an injured limb. While the results may be useful to evaluate the impact of injury on completing every day functional tasks, caution should be taken when attempting to apply findings to overhead throwing performance. Overhead throwing is reliant on the interaction of muscles through the KC, and the functional tasks investigated do not engage the core musculature or reflect the intensity of a maximal throwing motion.