


INTRODUCTION
Postural control, a fundamental motor ability developed during childhood, is crucial for independent mobility. However, postural control deficits – with varying degrees of severity – are highly prevalent in different pediatric disorders and even in some children without any formal diagnosis.1–3 To gauge the extent of these issues, their effect on motor function, and the success of therapeutic treatments, standardized tools for assessing postural control are necessary.4
Performance-based postural control tests are standardised assessments that evaluate postural control during functional movements.5 These tests can be conducted independently or as part of broader test batteries, assessing the various aspects of postural control or overall motor skills. Examples of general motor skills assessment batteries for children that include performance-based postural control subtests are the Movement Assessment Battery for Children – Second Edition (M-ABC2), the Bruininks-Oseretsky Test of Motor Proficiency (BOT) and Körperkoordinations Test für Kinder (KTK).6–8
Despite the abundance of performance-based tests and subtests, their systematic implementation in clinical practice remains low.9,10 Physiotherapists and other allied health care providers often cite a lack of time as a major barrier to the frequent use of standardized assessment tools.11 Furthermore, there is limited information on the psychometric properties of performance-based postural control tests.12,13 Proper training is essential for therapists administering these tests, as they often require multitasking skills such as providing correct instructions, tracking time, repetitions, and evaluating movement quality.
The results collected through performance-based postural control tests can thus comprise both simple (such as time measurements and number of repetitions) and complex data (such as qualitative assessment of posture and compensatory movements). While computer-assisted assessments have faced challenges in reliably and validly registering complex data, they have shown higher levels of agreement with face-to-face assessments for simple data.14,15 By delegating the registration of simple quantitative data to digital tools, clinicians can focus on evaluating more complex qualitative data. However, developers must ensure that these digital tools have the necessary psychometric properties, as clinicians rely on their accuracy.
Recently, there has been a notable increase in the development and research of rehabilitation technologies, particularly in the field of game-based interventions (exergames). These interventions have proven to be effective supplements to conventional physiotherapy, offering a more engaging and motivating option for patients.16 Though initially developed for non-clinical users, commercial exergaming devices like Microsoft Xbox Kinect and Nintendo Wii have shown promising results for both postural control assessment and training.16–19 However, the everchanging nature of the gaming market has led to the discontinuation of support and development for these movement-based devices by commercial companies.20 Rehabilitation technology specifically tailored for clinical physiotherapy practices could address this gap.
The pressure-sensitive device known as the ‘Matti’ (Creative Therapy, Belgium) was developed to capture movement data using a grid of resistance-based pressure sensors. Additionally, it can offer visual cues to users through a grid of integrated LED-lights. This interplay between visual elements and the pressure sensors enables the software to create interactive gameplay experiences.21 Beyond its use for exergaming, Matti has the potential to be used for digital performance-based postural control tests. Specifically, it can digitally record parameters related to duration or the number of correct performances. Automatic registration of these simple parameters could reduce the level of multi-tasking required by the examiner, resulting in more objective and accurate results, potentially enhancing the psychometric properties of the test. Additionally, incorporating interactive digital elements during testing might improve the examinees’ engagement or even enjoyment compared to traditional testing methods.
To determine Matti’s feasibility as a measurement device, this cross-sectional study explores three specific research goals. The first was to investigate Matti’s ability to accurately record two continuous parameters (time and number of repetitions) during the digitized implementation of two performance-based postural control subtests: The One-Board Balance Test (OBBT) from the M-ABC26 and The Lateral Jump Test (LJT) from the KTK,7 (Dutch version) in typically developing, active children. The second goal was to examine the relationship between observed and digital outcomes of the digitized test condition. The third goal was to evaluate whether this digitized assessment is perceived as more enjoyable by the children. Therefore, the purpose of this study was to examine the feasibility and validity of the Matti, a pressure-sensitive device, as a tool for recording simple continuous data for two performance-based postural control subtests: the time in seconds during the One-Board Balance Test (OBBT) and the number of jumps during the Lateral Jump Test (LJT), in typically developing children.
METHODS
Participants
Typically developing, active children, aged between seven and 12 years, were recruited through regional schools and recreational sport clubs. The 12-year cut-off was based on the maximum age for which the KTK is available,7 while the lower cut-off was based on the minimum age of Age Band 2 (7-10y) of the M-ABC2.6 Informed consent was provided by parents or a legal guardian prior to testing. Ethical approval was provided by the Ethics Committee of the University Hospital Ghent (BC-10697).
Procedures
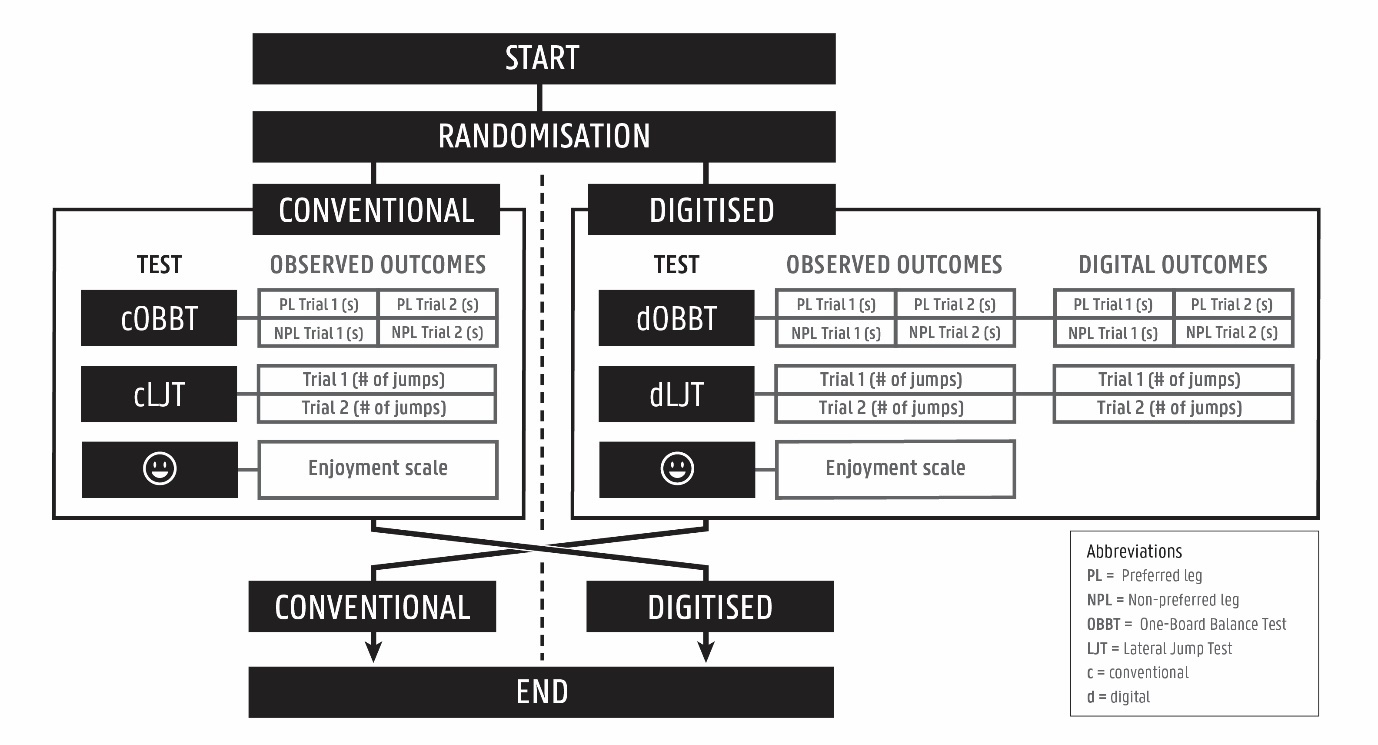
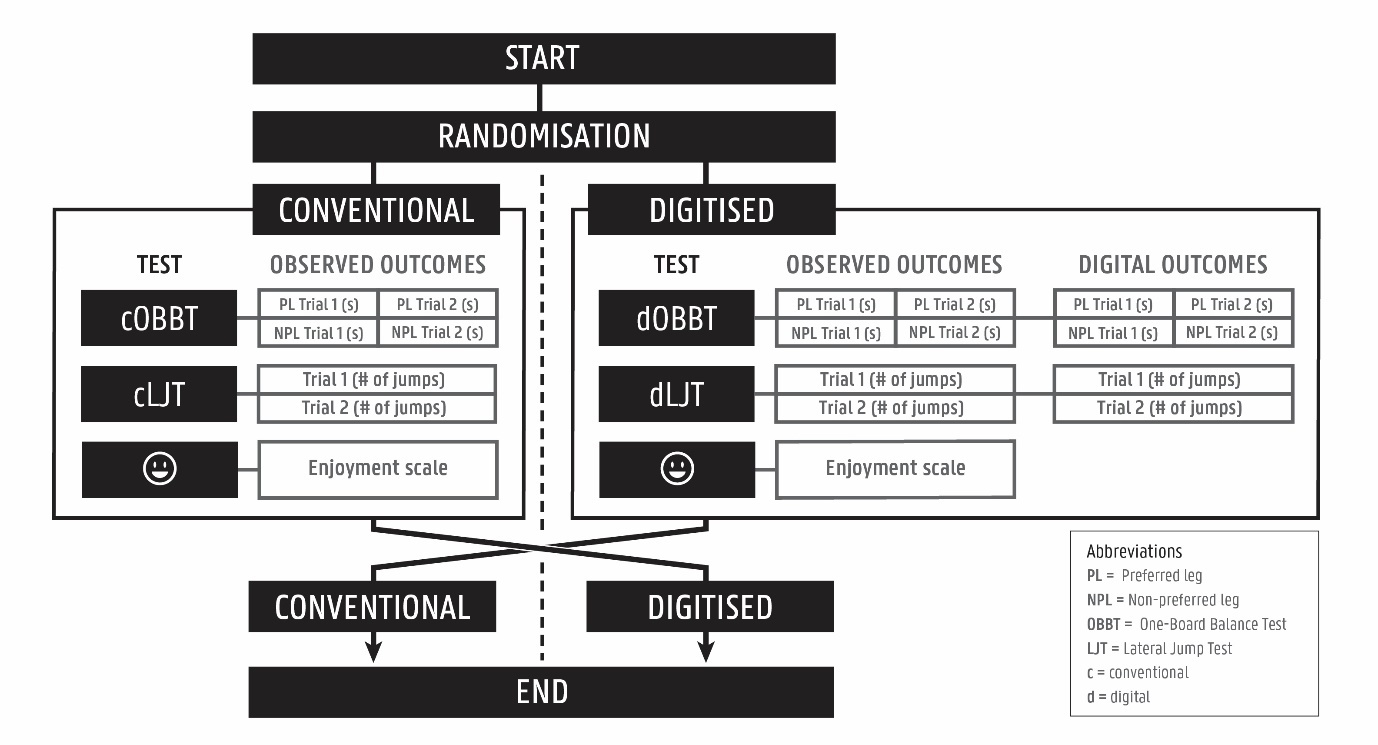
For this cross-sectional study, all participants were tested during a single session with both the conventional OBBT (cOBBT)6 and LJT (cLJT),7 as well as digitised versions of the OBBT (dOBBT) and of the LJT (dLJT) developed on the Matti system. Assessments were conducted by three graduate physiotherapy students specifically trained in the administration of both tests and supervised by a trained physiotherapist and researcher who was responsible for managing the Matti device and software. Prior to testing, the participants’ age, sex, and preferred leg were documented. Testing followed a single-session cross-over design whereby pairs of participants were tested simultaneously with one commencing with conventional testing, the other with digital testing (Figure 1). Starting conditions were randomized by letting one of the participants draw lots. To avoid any distractions during testing, both conditions were visually separated. Enjoyment of participants was evaluated using a 5-point Likert Scale with smileys representing the different degrees of boredom and enjoyment (Smiley-o-Meter,22 Appendix 1). After both tests were concluded and enjoyment was scored, the participants switched conditions.
Conventional testing
Conventional One-Board Balance Test
The cOBBT is a designated postural control test for children between seven and 10 years old. Unipedal stance is evaluated by measuring how long (in seconds) the child can maintain balance while the balancing foot is placed on top of a T-shaped balance board, specific to the M-ABC2. The maximum score is 30 seconds and both legs are tested up to two times. When the child can reach the 30 second mark with one side in one attempt, the trial is not repeated for this leg. The non-supporting foot is lifted to the back of the body by flexing the knee. If the balance board tilts, such that one of the sides touches the floor, the test ends immediately. If the child’s non-supporting foot touches the floor, or pushes it against the extended leg for support, the test also ends. The highest score, expressed in seconds (maximum of 30 seconds) obtained by each individual leg was extracted and used for data analysis in this study.
Conventional Lateral Jump Test
The goal of the cLJT is to cross a small wooden beam (60 x 2 x 2 cm) - placed on the centreline of a 100 x 60 cm rectangle – as many times as possible during 15 seconds by performing bipedal sideway jumps. This test is performed twice (with at least 10 seconds between the two trials) after which the summation of both results is used for scoring. In this study, the highest score, expressed in number of jumps, of either performance was extracted and used for data analysis.
Digitized testing
The interactive surface of the Matti functions as a tangible user interface allowing users to play exergames via a digital platform, which is run on an external laptop. The pressure-sensitive area on Matti measures 1.2 m² and contains a grid of 56x56 resistance-based pressure sensors. On top of this layer of sensors, a grid of 18x18 LEDs is built, allowing for the device to convey real-time and interactive visual information to the user. This final layer is topped with a sheet of LED-foam (translucent Polyurethane foam, 5 mm) which allows the transfer of LED light while providing the user with a soft and comfortable surface.
Digitized OBBT
For the dOBBT, the Matti only registered the time of unipedal contact. A rectangular area marked by LED lights in the centre of the device, showed where the balance board was to be placed. This rectangle acted as one active area (A), while the remaining surface of Matti acted as a separate active area (B). Once participants assumed unipedal stance on the balance board (resulting in pressure on A, none on B), the Matti automatically started to track time while continually highlighting area A in green (Figure 2A). On the external screen, this tracking process was visible in real-time. As soon as the Matti registered any pressure on area B (either by the placement of the non-supporting foot, or tilting of the balance board), tracking was stopped, the LEDs inside area A became red, the trial was concluded, and the final time in seconds was saved.
Digitized LJT
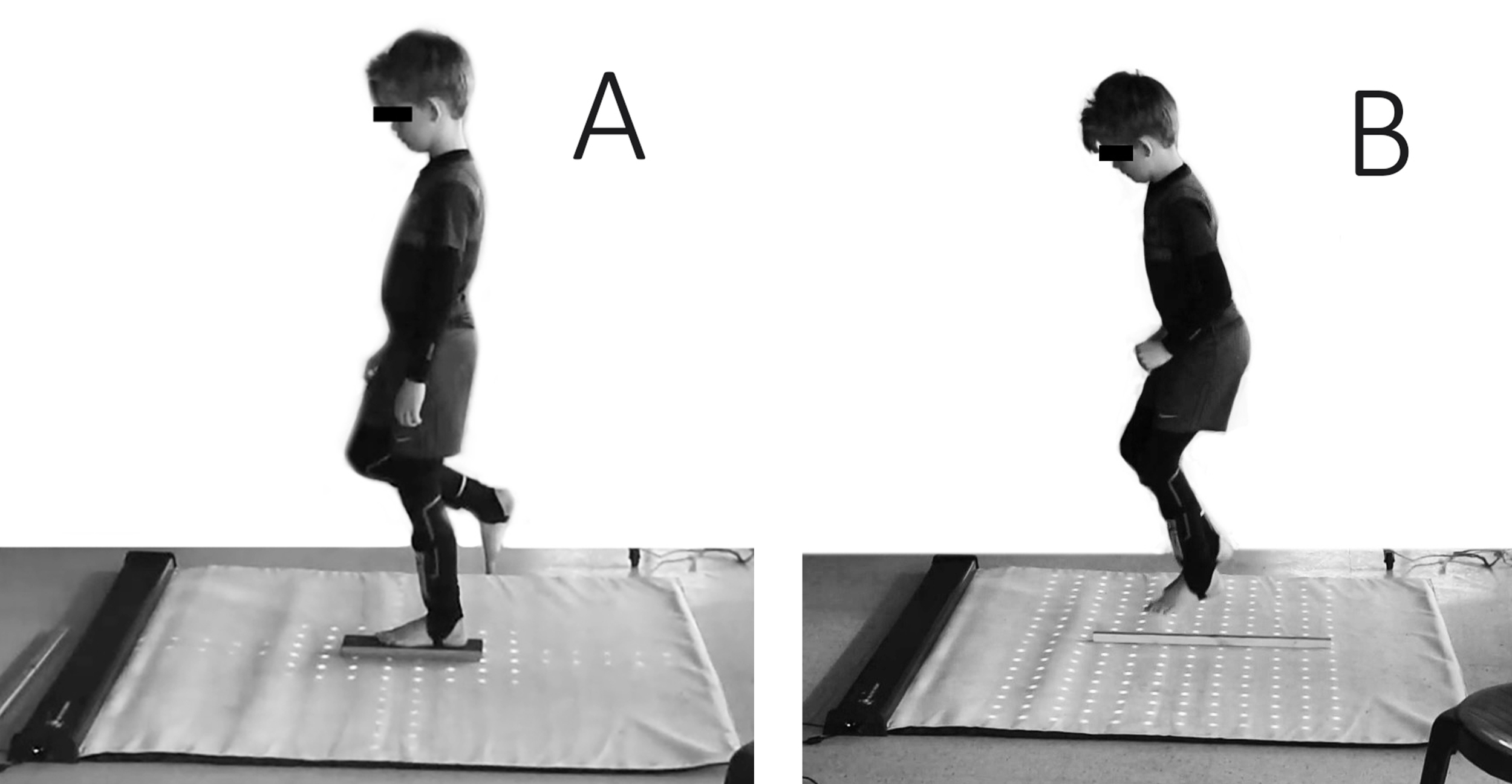
For the administration of the dLJT, the same wooden beam used in cLJT was placed in the centre of the Matti. A large horizontal rectangle of white LED lights highlighted the active areas for this test to the participant (Figure 2B). To score this test, the Matti defined two active areas: ‘L’ on the left side of the beam, and ‘R’ on the right. After a three-second countdown, shown on screen and vocalised by the administrator, Matti started registering each jump by counting the alternating pressure in zone L and R. After 15 seconds, the software stopped its count, and the trial was concluded.
Data analysis
Data were organized and annotated using Microsoft Excel, and analysed using SPSS Version 29.0 (SPSS Inc., Chicago, IL, USA). For the analysis, the highest score from both the preferred and non-preferred foot of the cOBBT and dOBBT was considered, along with the highest score from both trials of the cLJT and dLJT. The relationship between the digital and observed outcomes during digitized testing was analyzed by matching the highest digital score with the corresponding observed result. If a technical error was noted during one of the digital trials it was removed prior to analysis and the corresponding data point registered by the observer was also excluded. Data normality was examined using the Shapiro-Wilk Test. The relationships between observed dOBBT and cOBBT outcomes were investigated by calculating the Spearman correlation coefficient while systematic differences between test outcomes were examined using the Wilcoxon Signed-Rank Test. For the dLJT, relations between observed and digitized outcomes were evaluated using the Pearson correlation coefficient and paired sample t-tests. Interpretation of the correlation coefficients used the convention proposed by Chan: [< .30] poor or no relationship, [.30 - .59] fair; [.60 -.79] moderate; [≥ .80] very strong.23 When no statistically significant difference was found between the observed and digital outcomes of digitized testing, their level of agreement was examined using Bland-Altman plots. Finally, a signed Wilcoxon Rank Test was used to determine whether the enjoyment level of the participants was significantly different between the digital and conventional testing methods.
RESULTS
Forty-six typically developing children (36 males, 10 female) with a mean age of 8.98 (±1.04) years old were tested. Forty-one participants considered their right foot to be dominant. The data of the non-preferred leg OBBT for 1 participant and from the LJT of 8 participants were excluded from analysis due to technical errors or erroneous performance by the participant. Therefore, in total, 19 and 27 individual data-points were excluded from the dOBBT and dLJT datasets respectively. In addition, Smiley-o-Meter data of eight participants were missing. An overview of all omitted and missing data can be found in Appendix 2.
Table 1 provides descriptive statistics, correlation coefficients for the OBBT and LJT, and test comparisons.
One-Board Balance Test
No signidicant correlation between cOBBT and dOBBT scoring was found for the non-preferred leg (rs =.185, p=0.225) while a fair significant positive correlation was found for the preferred leg (rs =.471, p<0.001). Furthermore, dOBBT scores were significantly lower than the cOBBT scores for both the preferred (median cOBBT 24.30s (IQR 18.50) vs dOBBT 14.13s (IQR 20.88), p=0.004) and non-preferred leg (median cOBBT 23.34s (IQR 19.44) vs. dOBBT 13.39s (IQR 19.13), p=0.008).
Very strong positive correlations were observed between the digital and observer-based scoring of the dOBBT for both the preferred (rs=.991, p<0.001) and non-preferred leg (rs =.995, p<0.001). No significant differences between the digital and observer-based scoring of the dOBBT were found. The Bland–Altman plots for these comparisons displayed an even dispersion relatively close to their respective mean difference with only three outliers for the preferred leg measures, and two for the non-preferred leg (Figure 3).
Lateral Jump Test
For the LJT, a significant strong positive correlation (r=.723, p<0.001) between the cLJT and dLJT scores was found with no significant systematic difference between the test condition scores. While a significant and very strong positive correlation (r=.962, p<0.001) was found between the digital and observed outcomes of the dLJT, digital dLJT outcomes were also found to be significantly higher than those scored by an observer (dLJT 32.2 4± 4.61 vs. dLJT(obs) 31.79 ± 4.58, p =0.036).
_observed_vs._digital_outcomes.png)
Based on the results of the Smiley-o-Meter scores, children reported significantly higher levels of enjoyment during digital testing, compared to conventional testing (Z=-2.530; p = 0.011).
_observed_vs._digital_outcomes.png)
DISCUSSION
The feasibility of the Matti device was confirmed to register simple continuous parameters (in seconds and number of jumps) during digitized testing during two different performance-based subtests for postural control in typically developing children. When the OBBT and LJT were performed on the Matti, simultaneously generated digital and observer-based scores were highly correlated and resulted in similar results. Concurrent validity between conventional and digital test scores varied between subtests. While a moderate correlation between cLJT and dLJT was found, the correlation between cOBBT and dOBBT was fair for the preferred leg, and poor for the non-preferred leg. This implies that even though Matti might be able to accurately capture quantitative data, results on the digitized implementation of the performance-based ‘criterion’ test differed from the results of conventional test conditions. However, these differences are heavily dependent on the type of performance-based test and the type of parameter the Matti is measuring. Finally, the children who participated in this study reported higher levels of enjoyment during the digitized tests than during conventional tests.
Although current results indicate that Matti is able to measure the performance time of typically developing children on the dOBBT as accurately as an observer, five outliers were identified on the Bland-Altmann plots. All but one of these outliers stem from a higher digital score (measured by the device) compared to the score of the observer. This could indicate that the instrument still misses some modicum of error which the observer was able to pick up. These findings further highlight the importance of supervision by a clinician during testing, in order for them to make final call on the correctness or representativeness of the measurement.
Digital LJT results measured by the Matti showed very strong correlations with the simultaneously observed scores. While comparison of the mean number of jumps showed a systematic bias with more jumps recorded by the Matti, the average difference was <0.5 jumps. One explanation for the slightly higher number of jumps recorded by the Matti could be the software-based architecture of the dLJT itself. Since the Matti records the number of jumps through the alternating interaction with only two active areas it is unable to gauge the correctness of these jumps. While the test requires bipedal jumps, participants sometimes still end up jumping in such a way that they land with one foot on either side of the wooden beam. Though an observer might ignore this jump in their count, as long as both areas are touched in an alternating way, the Matti will still count this as a ‘correct jump’. Future improvements in the Matti software should be able to help in overcoming these issues by implementing more advanced algorithms to count the number correct jumps, while ignoring incorrect jumps.
However, the differences between the conventional and digital testing indicate that, for both the OBBT and LJT, the Matti insufficiently mimics its conventional counterpart. The foam surface of the Matti seems an important factor to be considered, especially given its interference with the stability of the balance beam thus increasing the difficulty of the dOBBT compared to the cOBBT. As such, the normative data available for the OBBT and LJT cannot be used for the digital test results. Since the isolated results of the OBBT and LJT are clinically meaningless without these standardized scores, the digital test results at present do not allow the clinician to adequately compare individual performances with peers of the same age and sex. Further data collection in typically developing children and populations with underlying pathologies could allow for further development of these tests, including the collection of standard scores.
Digital testing might introduce extra variables. New normative data or standard scores should therefore be collected independently from their corresponding conventional testing manuals. The resulting data will however be tied to the digital device used, potentially limiting usability for therapists. Various factors, including clinician circumstances and market trends, could render normative data development efforts obsolete. The rise and fall of the commercial exergaming consoles Nintendo Wii and Xbox Kinect are exemplary to this issue. Though extensively investigated, both systems have been discontinued by their respective developers.16,20 Solutions such as the Matti device, specifically developed for use in a clinical context, may offer a more long-term platform for the implementation of digitised testing in physiotherapy practices.21,24
Nevertheless, these digital tests appear to be more enjoyable, potentially providing extra engagement and motivation for the patient, and merit further investigation as postural control tests. Overall, the digitized test seemed to be favored over conventional tests by participants. Moreover, some children specifically noted an increase in comfort during the dLJT due to the foam surface of the device, while others liked the fact that the interactive LED-lights offered some form of feedback during testing. On the other hand, these same elements were a source of frustration for other participants who felt the foam surface made the dOBBT more difficult or found the LED-lights somewhat distracting.
Limitations and future research
While digital postural tests should certainly be explored, some important caveats need to be addressed. The first limitation is that this study only used two small sub-tests from different motor function assessment batteries.6,7 Comprehensive postural control tests like the Pediatric Balance Scale and Kids BESTest typically include multiple sub-tests measuring various parameters.25,26 Digitizing entire test batteries could be a better strategy for developing digital postural control assessment devices.
A second limitation is the fact that individual conventional tests come with their own limitations, such as ceiling effects in older children.26,27 Digital alternatives could provide more accurate and sensitive assessments of various aspects of postural control. To highlight these potential benefits, future research should evaluate these new devices both in- and outside the lab, using pragmatic trials which reflect the actual context in which these tools will be implemented.28
A third limitation resulted from the stringent COVID-regulations which were in effect during testing. This study was conducted at three separate test locations over four different days. While this allowed for the recruitment and assessment of more participants, some concessions to standardisation of environments were necessary. A specific example was the separation of conventional and digital test areas. Only at one site were the researchers able to completely separate both conditions by utilizing two separate rooms. At the other locations, the researchers had to construct a separating element themselves, allowing for the visual separation of both test areas. Additionally, inter-rater reliability was not investigated during this study, yet has been previously reported to be high for the conventional test condition of both the OBBT and LJT with some caution regarding variations in the OBBT.29–32
As a fourth limitation, this study only assessed postural control in typically developing children who regularly attended sports training. As found by previous research, active children and adolescents show different or even better posture control strategies than their inactive peers.33,34 Future research should strive to broaden the sample population to both active and non-active children, and children with underlying pathologies which may affect postural control. Ultimately, the collection of standard scores could allow for the interpretation of test results.
The fifth limitation is that even though data analysis on the Smiley-O-Meter showed significantly higher levels of enjoyment during digital testing, these results should be interpreted with some caution. As shown by previous studies, children between eight and 10 years are limited in their ability to self-monitor,35 and can often like or even pretend to like what is presented to them in order to please the inquiring adult.36 Expressions and reactions of the participants during testing also painted a more nuanced picture. A single Likert scale (e.g. the Smiley-O-Meter) might thus be insufficient to accurately gauge the levels of enjoyment in children. To ascertain the positive trends shown by our results, future studies should aim to include more robust and in-depth analysis tools to assess the levels of enjoyment experienced by children during a specific task. The addition of qualitative and structured interviews might aid future researchers to specifically identify what aspects of digital testing children find more enjoyable when compared to conventional tests.
A sixth and final limitation was the issue whereby some data points were lost due to technical errors in the measurements of the Matti device. While technological devices are always susceptible to certain types of bugs in their hard- or software, efforts should be made to keep these errors to a minimum, especially in devices meant for clinical use. Fortunately, most of the technical errors encountered during this study were a result of certain decisions in the coding of the software (e.g. time-out time when jumping on the wooden beam during dLJT). By their nature, software bugs are easier to correct and can be rapidly implemented for all users. Future research should thus focus on identifying minor and major bugs, while close collaboration between developers, engineers, clinicians, and researchers could allow for rapid and useful iterations of design.
CONCLUSION
By accurately measuring time spent on one leg in typically developing children, the Matti – a pressure-sensitive exergaming device – could be of added value during a OBBT test allowing the examiner to focus on the more complex qualitative aspects of postural control. However, these digitally acquired scores cannot be used to calculate standardized norm scores since participant scores obtained during this digitized version of the OBBT were significantly lower than their scores on the conventional test.
The Matti-based dLJT results showed strong correlations with simultaneous observer-based results, thus showing potential to automate the quantitative aspects of the LJT. Any overestimation of jumps registered by Matti during the dLJT was likely due to a programming error which can be resolved through modifications in the software. Therefore, it is likely that the LJT could be digitized allowing for a more qualitative observation by an examiner.
These results thus indicate that the Matti device appears a feasible tool to accurately measure time- and frequency-based parameters during digitalised versions of the OBBT and LJT. While the concurrent validity between the conventional and digitized version of these tests could not be proven, the participants’ perceived enjoyment of the digital testing merits further investigation of digital postural control testing tools. Additional improvements to the test setup and the development of digital-specific postural control tests will be necessary to achieve this.
Corresponding author
Anke Van Bladel
Universiteit Gent
Faculteit Geneeskunde en gezondheidswetenschappen
Vakgroep Revalidatiewetenschappen,
Campus UZ Gent
Gebouw B3
C. Heymanslaan 10 9000 Gent
E-mail: Anke.VanBladel@UGent.be
Phone: 09 332 46 57
Funding
This research was funded by Flemish funding agency VLAIO under agreement HBC.2020.2294. The project HBC.2020.2294 had a contract between Ghent University and Creative Therapy for the execution of the project. Jorn Ockerman is employed by Creative Therapy under the conditions of the agreement. Jelle Saldien is co-founder, shareholder and member of the board of Creative Therapy