INTRODUCTION
Soccer has steadily risen in popularity, attracting active males and females worldwide. Specifically, soccer participation among adolescent females has experienced exponential growth, attributable in part to increased media coverage, greater investment in women’s sports, and the rising visibility of professional female athletes.1 However, as sport participation rises, so does exposure to injury.2,3 Female soccer players are two to nine times more likely to experience an anterior cruciate ligament (ACL) injury compared to males, with approximately 18% of high-level women’s soccer players having a history of ACL injury.4 Therefore, a strong understanding of the biomechanical risk factors associated with ACL injury,5 particularly those specific to soccer movements, is important for developing effective strategies to reduce injury risk in female athletes.
Soccer athletes perform highly dynamic movement patterns that require speed, strength, and agility, such as sprinting, changing direction, jumping, and kicking. While these movements are an important aspect of high-level performance, poor technique can quickly increase the risk of injury. Notably, female athletes have been found to have high-risk knee mechanics, such as increased dynamic knee valgus, specifically during cutting, pivoting and landing movements that have been shown to increase load on the ACL and thus heighten the rate of injury compared to males.6–9 During a soccer kick specifically, prior research has primarily investigated varying positions of the swing limb,10 angle of the stance foot,11 and approach angle when kicking to increase movement efficiency.12,13 However, limited investigations have focused on the mechanical contributions to potential risk factors associated with the stance limb during kicking, despite the stance limb bearing substantial load throughout kicking.
In the current study, strike stance angle (SSA) was used to assess the orientation of the stance limb in relation to vertical when kicking, which can be useful in identifying potential biomechanical risk factors associated with the loaded limb. The stance limb of a soccer player is loaded multiple times during a game. While a direct causal link between SSA and ACL injury risk has yet to be established, coronal plane deviations of the lower limb have been associated with altered joint loading and injury risk factors.14 Therefore, assessing coronal SSA may provide insight into how improper loading mechanics during kicking may relate to potential risk factors of injury. Specifically, the purpose of this study was to quantify the relationship between SSA and lower extremity kinematics and kinetics during a soccer kick. It was hypothesized that a greater SSA would be correlated to greater biomechanical risk factors and that correlated findings would differ by dominance. Understanding the role of SSA in kicking mechanics can contribute to more effective training protocols for female athletes, optimizing stance position to reduce risk factors potentially leading to injury. Findings from this study may lead to evidence-based recommendations for improving soccer kick mechanics and reducing lower extremity injury risk in female soccer athletes.
MATERIALS AND METHODS
Participants
Participants tested for this study consisted of healthy female youth athletes who reported soccer as their primary sport. Participants were excluded if they reported a lower extremity injury six months prior to testing, or any musculoskeletal or neuromuscular conditions that would prevent their abilities to complete the soccer kick task. All participants wore their preferred athletic footwear and attire during testing in the motion capture laboratory. This study was approved by the local Institutional Review Board, and informed consent/assent was obtained from all parents and participants prior to participation.
Tools and Equipment
A 14-camera motion capture system (Vicon Motion Systems Ltd, Denver, CO, USA) was utilized to collect kinematic data at 240 Hz. Retroreflective markers were placed on anatomical landmarks on the trunk, pelvis, thigh, shank, and foot derived from the Modified Helen Hayes marker set.15,16 Specifically, trunk markers were placed on the first and tenth thoracic vertebrae, jugular notch, mid-sternum, xyphoid process, and sacrum. Additionally, markers were placed bilaterally on the anterior superior iliac spines, medial and lateral femoral epicondyles, patella, anterior shank, medial and lateral malleoli, heel, first metatarsal, and fifth metatarsal. Fixed marker clusters were placed bilaterally on the anterior shank and lateral thigh to aid in overall lower extremity tracking. Six embedded force plates (Advanced Mechanical Technology, Inc., Watertown, MA, USA) were used to collect kinetic data at a sampling rate of 2,880 Hz.
Task Procedures
Participants completed four trials of soccer kicks, two kicks per leg. The athlete’s typical kicking leg was recorded as their dominant limb and used for comparison to the non-dominant limb. However, to provide context for interpretation, when referring to findings for the “dominant kick”, kinematics and kinetics were presented for the stance limb. The kicking task was completed in a 15-foot stretch of space on the floor of the laboratory, including a large net to replicate a soccer setting. There was sufficient space leading up to the force plates where participants could approach the ball as they typically would when performing a penalty kick. Participants were instructed to kick as they normally would, and their starting position was adjusted, as to not alter their natural kicking mechanics, such that their stance/plant limb landed on the force plate while performing the soccer kick. Trials in which the participant did not plant solely in the force plate were deemed unsuccessful and discarded.
Data Processing and Analysis
Kinematic data were processed in Vicon Nexus software and were filtered using a Woltring filter (predicted mean square error of 10 mm2). Kinetic data from the force plates were also processed in Vicon Nexus software and filtered using a fourth-order low-pass Butterworth filter with a cutoff of 16 Hz. A custom MATLAB (MATLAB 2022a, Natick, Massachusetts, USA) code was used to determine joint and segment angles and (external) moments in the sagittal, coronal, and transverse planes. The hip joint centers were estimated using the Harrington method, while the knee and ankle joint centers were calculated as the midpoint between the respective medial and lateral joint markers.17 Segmental angles and moments were subsequently extracted at the time of ball contact during each kicking trial. Ball contact was defined as the timepoint where the swing and stance limbs were adjacent using the difference between the toe markers, tracking where the ball would be impacted. Entry velocity was also calculated using a custom MATLAB code, taking the maximum velocity from the sacrum marker between the previous contralateral step and initial contact of the stance limb.
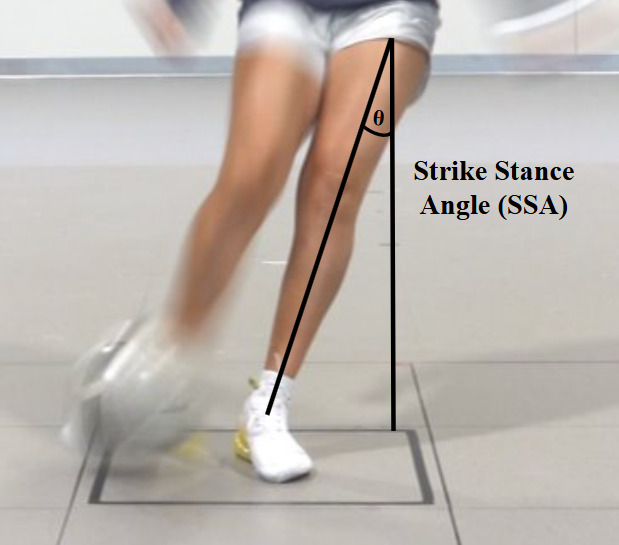
Lastly, SSA was calculated at the time of ball contact to assess the alignment of the stance limb in the coronal plane of the global coordinate system (Figure 1). SSA was defined as the two-dimensional angle between the vector connecting the stance limb’s hip joint center and ankle joint center and the vertical axis of the global coordinate system, projected into the coronal plane of the of the global coordinate system. To ensure consistent interpretation across kicking sides, the SSA was sign-adjusted such that a positive angle represented medial inclination of the stance limb, regardless of whether the left or right limb was used for stance. Additionally, swing limb speed was calculated using the three-dimensional position of the ankle joint center in the global coordinate system. The linear displacement vector was measured by subtracting the ankle joint center position at ball contact from that at initial contact. The magnitude of this displacement was divided by the elapsed time between the two events to compute swing limb speed (m/s). Of the successful trials, the trial with the fastest entry velocity was chosen for each kicking limb and used for subsequent analysis.
_at_ball_contact.png)
Given significant tests for normality (Shapiro-Wilk), nonparametric analyses were conducted using the Wilcoxon signed-rank test. Spearman correlations were performed to identify significant relationships between SSA and kinematic and kinetic measures for both stance limb-dominant kick and stance limb-non-dominant kicks at ball contact. To address multiplicity, the false discovery rate was controlled using the Benjamini–Hochberg procedure with Q = 0.10. Corrections were applied within families of tests that addressed distinct questions: (a) limb-to-limb comparisons and (b) correlations between SSA and kinematic and kinetic variables. Only FDR-adjusted p-values are reported, and inferences are based on these adjusted values. For transparency, rank-based effect sizes (r) with 95% confidence intervals are also reported for paired comparisons. Lastly, correlation strengths were defined as weak (r ≤ 0.35), moderate (r = 0.36-0.67), or strong (r ≥ 0.68).18
RESULTS
Nineteen healthy female soccer players (15.2 ± 0.9 years, 168.2 ± 5.8 cm, 61.3 ± 7.8 kg) were tested from October 2023 to August 2024 in which they performed soccer kicks bilaterally. All participants reported their right leg as their dominant limb that they preferred to kick with. A total of 37 soccer kicks were included for correlation analysis, as one kick was removed from the dataset due to an incorrect execution of the task. No significant differences between stance limb-non-dominant and stance limb-dominant kicks were observed for kinematic and kinetics at ball contact. Spearman correlation results between SSA and dominant and non-dominant kick kinematics and kinetics are presented in Table 1. Detailed descriptive data and statistical results, including effect sizes, are presented in Appendix A.
Performance Metrics
For both the dominant and non-dominant kicks, there were no significant correlations between entry velocity and SSA. On the non-dominant kick, greater swing limb speed was moderately correlated with SSA (r = 0.55 p = 0.038). There were no significant correlations between SSA and swing limb speed during the dominant kick.
Trunk and Pelvis
There were no significant correlations between trunk and pelvis measures and SSA at ball contact during the stance limb-dominant and stance limb-non-dominant kicks.
Hip
There were no significant findings between hip kinematics and kinetics and SSA during the stance limb-non-dominant kick. On the stance limb-dominant kick, greater hip adduction was moderately correlated with a greater SSA (r = 0.51, p = 0.261). Thus, as the stance limb plants at a greater angle, the ipsilateral hip becomes more adducted. While there was a relatively moderate correlation, it was not statistically significant.
Knee
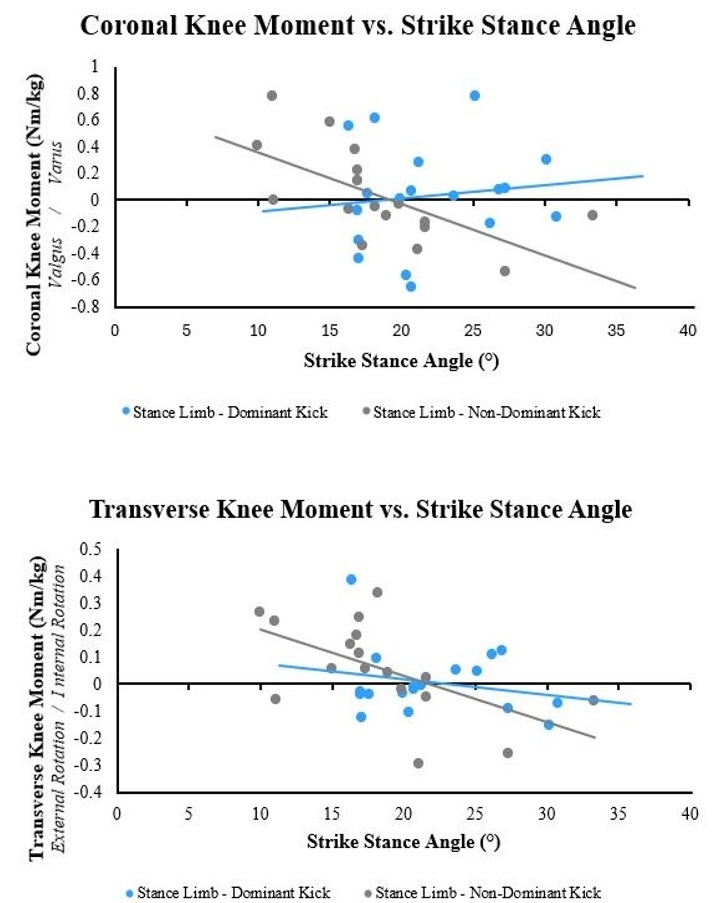
On the stance limb-non-dominant kick, increased knee flexion correlated with a greater SSA (r = 0.48, p = 0.264). While this is a relatively moderate correlation, it was not statistically significant. SSA was found to have a strong negative correlation with coronal knee moment (varus moment) (r = -0.81, p = 0.002), such that a greater SSA was associated with a reduced knee varus moment, or in some cases a greater knee valgus moment, on the stance limb during the non-dominant kick at ball contact (Figure 2). The transverse moment at the knee exhibited a moderate negative correlation to SSA (r = -0.66, p = 0.038), which indicates that a greater SSA is associated with a reduced internal rotation moment, or in some cases an increased external rotation moment, at the stance limb knee during the non-dominant kick (Figure 2). Similarly, knee flexion during the stance limb-dominant kick was moderately correlated with SSA (r = 0.50, p = 0.261). This indicates that as the SSA increases, there is more flexion on the stance limb at ball contact. Although the correlation was moderate, it was not statistically significant.

Ankle and Foot
A strong positive correlation was found between SSA and sagittal ankle angle (r = 0.72, p = 0.018) during the stance limb-dominant kick, indicting that as SSA increased, ankle dorsiflexion also increased at ball contact. There were no significant correlations between SSA and foot rotation during both the stance limb-dominant and stance limb-non-dominant kicks.
DISCUSSION
The results of the current study defined the relationship between SSA and lower extremity kinematics and kinetics at ball contact during a soccer kick in adolescent females. The hypothesis, that a greater SSA would be correlated to greater biomechanical risk factors differing by dominance, was supported. Biomechanical measures with the strongest associations to greater SSA for the stance limb-non-dominant kick were increased knee valgus moment and knee external rotation moment. For the stance limb-dominant kick, the strongest association to greater SSA was increased ankle dorsiflexion, and non-significant trends existed toward associations with increased hip adduction and knee flexion at ball contact.
Although not statistically significant, the observed trend of increased hip adduction with greater SSA likely reflects compensatory mechanics arising from limited dynamic stability and coronal plane control at the hip. The observed trends approaching statistical significance may be attributable to the limited sample size and could reach significance in studies with a larger cohort. One study similarly found that soccer players exhibited greater hip adduction angles due to muscle shortening of the hip flexors as a result of habitual recruitment during a single-leg squat task, a common imbalance leading to altered hip mechanics.19,20 Hip adductor and abductor strength in both the swing and stance limb help stabilize the orientation of the body throughout the entire soccer kick, emphasizing the importance of maintaining hip strength to prevent imbalances that pose a risk for injury.21 Numerous reports have shown that females tend to have less hip abductor strength compared to males, indicating a potential association to dynamic knee valgus which may increase risk of ACL injury.22–24 Specifically, weak hip abductors may lead to an inability to prevent knee collapse into valgus. Similarly, in the current study, the association between greater SSA and hip adduction during the stance limb-dominant kick may indicate a deficit in hip abductor strength to control the entire movement. Previous research has identified that decreased muscle activation at the hip ultimately decreases quadriceps and hamstring activation in the stance limb.25 This reduction in activation limits the dynamic stability of the knee joint, putting the lower extremity at risk for injury. Additionally, it has been reported that females typically land from a jump in a more upright hip position, resulting in an altered knee angle upon landing that poses biomechanical risk factors.25 The results of the current study indicated that altered mechanics of the stance limb hip, and an upright position when establishing the stance limb at ball contact may improperly distribute the load throughout the kick. Incorporating hip abductor strength exercises into female soccer athlete’s training protocol to aid in dynamic stability may benefit players from both an injury prevention and performance standpoint.
In the present study, the significant increase in knee valgus moment with greater SSA suggests elevated mechanical loading at the knee, which may have implications for joint stability and injury risk during the soccer kick. Although not statistically significant, the observed trend toward increased knee flexion may also have potential relevance for altered joint loading and stability under these conditions and should be studied further. On average, the stance limb of a soccer player is loaded at least 20-25 times during a 90-minute game,13 and improper loading at the knee joint can predispose athletes to the risk of injury.26–28 Interestingly, a previous study investigated ground reaction forces of the stance limb during a soccer kick, suggesting that the soccer kick resulted in significant loading of hip, knee, and ankle joints.29 Repetitive loading on the stance limb with a greater SSA, alongside other biomechanical risk factors, may be putting the lower extremity in a vulnerable position at risk for injury. The current study identified several contributors to dynamic knee valgus – greater knee valgus moment, hip adduction, and external tibial torsion (via external knee rotation moment) – relating to greater SSA during a soccer kick. Therefore, a greater SSA may be associated with valgus loading, a biomechanical risk factor for ACL injury.5,30 Likewise, during a single leg squat task, investigation of the musculoskeletal profile of elite female soccer players revealed that many demonstrated a combination of hip adduction, hip internal rotation, knee valgus, and reduced knee flexion.19 Previous studies have investigated sex differences regarding knee valgus loading during dynamic tasks, suggesting that females land in greater knee valgus than males, a factor that contributes to the sex disparity in ACL injuries.31 Having a greater SSA in addition to predisposed knee valgus during a soccer kick may further increase the likelihood of injury in female soccer players due to the increased load on the stance limb knee joint.
Regarding limb dominance, the stance limb is the main contributor to stability and balance throughout the kick. When kicking with the non-dominant limb, this stability is often compromised due to less strength and control, which can put increased stress on the hip and knee joints.32 Additionally, less experienced athletes will typically only kick with their dominant limb, whereas high-level soccer players tend to be more symmetrical in strength and skillset. Due to the unfamiliarity of kicking with their non-dominant limb, they may have altered stance and kicking mechanics that are suboptimal to offset for the lack of strength and balanced force distribution. It has been reported that female athletes playing asymmetric sports exhibited greater dynamic balance in their dominant limbs compared to their non-dominant limbs.33 Greater emphasis on strength and balance training for the non-dominant limb in asymmetric sports is necessary to mitigate risk and further improve performance variables. Future studies with larger sample sizes may be able to identify greater biomechanical deficits between dominant and non-dominant limbs when kicking, however, limited research has been conducted on both limbs during a soccer kick.
Female athletes have also been shown to perform dynamic athletic maneuvers with decreased hip and knee flexion (i.e., stiffer landing strategies) as well as greater knee valgus moments.25,34,35 However, this trend was not fully supported in the current study given the association between increased ankle dorsiflexion and greater SSA in addition to observed trends toward increased knee flexion. These moderate to strong associations may be the result of compensating for weakness of the hip stabilizers, creating a greater range of motion in the hips to follow through, or for shock absorption to maintain balance throughout the kick. From a performance aspect, prior research has investigated how support limb kinematics were related to kicking performance in which a stiffer, more extended stance limb throughout each phase of the soccer kick was related to faster foot speeds at ball contact, which resulted in a higher contralateral hip position creating greater stance limb stability.36 The current study found that faster swing limb speeds during kicking were associated with a greater SSA in the non-dominant kick. This may reflect a compensatory strategy in high performance players to promote increased toe clearance and to accommodate for the demands of faster swing limb velocities. The increased SSA could be necessary to aid in maintaining balance and generate more power as the swing limb speed impacts the entire body. However, this biomechanical adaptation may also be linked to elevated injury risk as greater SSA can increase joint loading and compromise overall stability during the kick. As the current study did not investigate in-depth measures of performance but rather focused on biomechanical risk factors, future directions should focus on how SSA can influence performance variables, such as ball speed and kick accuracy, coinciding with stance limb kinematics.
Limitations
The current study has some limitations that should be noted. Given the current study was conducted on healthy, young female athletes, the results presented here may not be generalizable to older female or male participants. Adolescent females exhibit an increased risk for ACL injury, due in part to differences in lower extremity biomechanics, which has been well documented in prior works investigating dynamic athletic maneuvers.26,35–38 Thus, future work is needed to determine how sex or age may influence SSA associations as tested in the current study. Additionally, the laboratory setting and surface was not a typical representation of a game-like environment (i.e., field or turf). However, there was an ample amount of space for dynamic, free movements and a large goal to mimic the competition environment with the intention of having no variation in their natural kicking technique. Future studies examining associations between SSA and kinematic and kinetic measures should include different skill level athletes, uncontrolled conditions, such as kicking a moving ball, and more realistic surfaces such as turf or grass.
The current analysis was isolated to ball contact because SSA was defined at this event. While this event-focused approach preserved construct validity and limited multiplicity in a modest sample, it did not capture how pre- and post-contact mechanics may relate to SSA or performance. In addition, the authors were unable to quantify kicking accuracy as there was no ability to track the position of the ball as it reached the net. Future work will extend this initial analysis by investigating the relationship between SSA and both performance metrics and biomechanical risk factors observed across different phases of the kick to enhance applicability and clinical relevance.
Lastly, the sample size of the current study was modest (n = 19) relative to the number of variables analyzed, which increases uncertainty in estimates and raises the risk of both false positives and false negatives, particularly for correlation-based analyses. Although false discovery rate was controlled for at Q = 0.10 within families of tests and emphasized effect sizes with confidence intervals, the findings should be interpreted as exploratory and require replication in a larger cohort.
Conclusion
The findings of the present study highlight kinematic and kinetic associations with greater SSA, which included biomechanical risk factors differing between dominant and non-dominant limbs. Specifically on the stance limb-non-dominant kick, increased knee valgus and external knee rotation moments were found to be significantly associated with greater SSA. Conversely, a greater SSA on the stance limb-dominant kick showed a significant association with ankle dorsiflexion. Understanding the influence that SSA has on movement patterns when kicking should inform training protocols, allowing for a greater focus on both dominant and non-dominant limbs and optimizing kicking stance to promote injury prevention. Further research is needed to better define the relationships between SSA and lower extremity biomechanics of healthy youth soccer players during kicking, and to investigate its impact on injury prevention. Additionally, future work should identify how SSA can impact performance metrics, such as ball speed and accuracy, to provide a well-rounded training protocol that incorporates both injury prevention and performance aspects of soccer kicks.
Conflict of Interest Statement
The authors have nothing relevant to disclose.