INTRODUCTION
Rolling is a fundamental movement skill that humans develop in infancy and utilize throughout their lifespan.1 This coordinated movement requires muscular contributions from multiple body regions: upper extremities (shoulder flexion and horizontal adduction), core musculature (trunk rotation), and lower extremities (hip flexion and extension).1 Beyond its developmental importance, rolling is also critical for independence in adulthood and impaired rolling ability can lead to significant health implications including increased risk of pressure injuries in bed bound individuals.2 Various conditions can impact rolling ability, including neuromuscular diseases, Parkinson’s Disease, spinal cord injury, and advanced age.3–5
Assessing rolling ability has potential implications across diverse populations. In athletic populations, rolling assessment may provide insights into rotational power, core stability, and strength that impact sports performance and injury prevention.1 Rotational movements associated with rolling are crucial in athletic performance and provides a foundation for complex athletic movements by establishing core stabilization and coordinated extremity function.6,7 In rehabilitation settings, rolling and rotational strength assessment could also help track progress in patients with neurological conditions, after surgery, or advanced age.2–5 Additionally, rolling patterns might serve as an early indicator of movement dysfunction in otherwise healthy populations, allowing for preventive intervention to be performed before significant limitations develop such as knee injuries due to decreased hip abduction strength.1,8,9
Currently, numerous validated quantitative measures exist for assessing various aspects of physical function. These include tests for muscle strength (Medical Research Council Manual Muscle Testing),10 fall risk (Timed Up and Go),11 gait speed (10-meter walk test),12 balance (Berg Balance Scale),11 lower body strength and endurance (30 Second Chair Stand Test),13,14 core muscle endurance (maximum Plank Hold),12 and general mobility (Elderly Mobility Scale).15 While these established tests primarily assess movements in the sagittal plane, focusing on joint flexion and extension, there remains a notable absence of standardized evaluations for transverse and frontal plane movements, particularly those involving trunk rotation and hip abduction/adduction.
Despite rolling’s fundamental importance to both daily function and rotational movements for athletic performance, no standardized quantitative measure exists for assessing rolling ability and its relationship to muscle strength and endurance. Recognizing this gap, this study introduces the novel 30-second Roll to Quadruped test (30RQ), designed to measure rolling ability and its correlation with specific physical capabilities. Therefore, the purpose of this study was to determine if the 30-second Roll to Quadruped test (30RQ) can serve as a measurement of rolling ability and to explore relationships between participants’ rolling abilities, rolling strategies, strength, endurance, age, sex, activity levels, and BMI.
METHODS
Study Design and Participants
This cross-sectional observational study was approved by the Institutional Review Board for Human Subjects Research at the University where the authors are employed (IRB #5514). Nineteen healthy adults (8 males, 11 females) aged 20-40 years were recruited from a Doctor of Physical Therapy program through convenience sampling. Inclusion criteria consisted of: (1) age between 18-40 years, (2) no musculoskeletal injuries within the prior six months, and (3) ability to understand and follow testing instructions. Exclusion criteria included any recent injury or condition within the prior six months that would affect testing performance, an inability to understand and follow testing instructions, and being younger than 18 years of age or older than 40 years of age.
Testing Procedures
All testing was conducted in a single session following a standardized protocol. After providing informed consent and completing demographic information (age, sex, activity level, height and weight to calculate BMI, and injury history), participants performed a five-minute warm-up on a stationary bike at a self-selected intensity targeting 5/10 on the modified Borg scale of perceived exertion. Activity levels were categorized as sedentary, lightly active, moderately active, highly active, and extremely active. Sedentary was defined as performing little to no exercise per week. Lightly active was defined as exercising 1-2 day per week. Moderately active was defined as exercising 3-5 days per week. Highly active was defined as exercising 6-7 days per week and extremely active was defined as exercising more than once daily. BMI was calculated by dividing weight (kg) by height (m)².
Strength Assessment
Upper extremity muscle strength testing was performed in supine and consisted of elbow flexion and extension, shoulder flexion, abduction, adduction, external/internal rotation, extension, and horizontal abduction/adduction. Lower extremity muscle strength testing was mostly tested in supine, but knee flexion/extension and hip internal/external rotation were tested in sitting.
All strength tests were assessed in a consistent order using a handheld force dynamometer (ergoFET Digital Force Gauge, Hoggan Scientific, LLC., Salt Lake City, UT, USA) according to the Hoggan Scientific, LLC muscle testing positions educational handout (Appendix 1). Researchers used verbal cuing and encouragement for the participant to perform at their maximum effort during the strength testing. Two measurements were performed for each movement per side with a five second isometric hold each time, and the average value of the two measurements was used for data analyses for each muscle group tested. Co-investigators assessed the right side and then the left side before taking the second measurement with a 30 second rest break in between the first and second measurement for the same muscle. All strength measurements that were tested in sitting were taken first, followed by the measurement tested in supine to reduce the number of changes of position by the participant. Mean maximum values between the right and left sides were used for data analysis.
Core Endurance Assessment
Following strength testing and a five-minute rest period, participants then performed a maximum duration plank test to assess their core endurance. The test was terminated by the co-investigator when participants could no longer maintain proper form (defined as holding a plank position on the toes and elbows on a mat with a straight back, hips straight, and knees straight) as visually determined by the examiner, or the participant voluntarily stopped.
30-Second Roll to Quadruped Test (30RQ)
After a five-minute rest period, participants performed the 30RQ test on a mat on the floor. Starting in the supine position with arms by their side, participants were instructed to roll alternately right and left into quadruped position (shoulder, hips and knees at 90 degrees) as many times as possible in 30 seconds. Each time the participant rolled into quadruped it was counted as one repetition. All participants were given time to practice prior to starting the assessment. Video recordings were taken from both sagittal and frontal planes to capture rolling strategies. A successful roll was defined as achieving proper quadruped position with shoulders, hips, and knees at 90 degrees before initiating the roll back to the supine position and then back to quadruped on the other side. The total number of rolls completed in 30 seconds were counted and recorded for each participant and were also categorized by rolling strategy.
Lower Extremity Endurance Assessment
Following another five-minute rest period, participants completed the 30-second Chair Stand Test (30 CST) to assess their endurance. Participants performed the 30 CST with their arms crossed over their chest, recording the number of complete sit-to-stand repetitions achieved from a standard 18-inch chair. This assessed the participants overall lower extremity endurance.13,14
Video Analysis
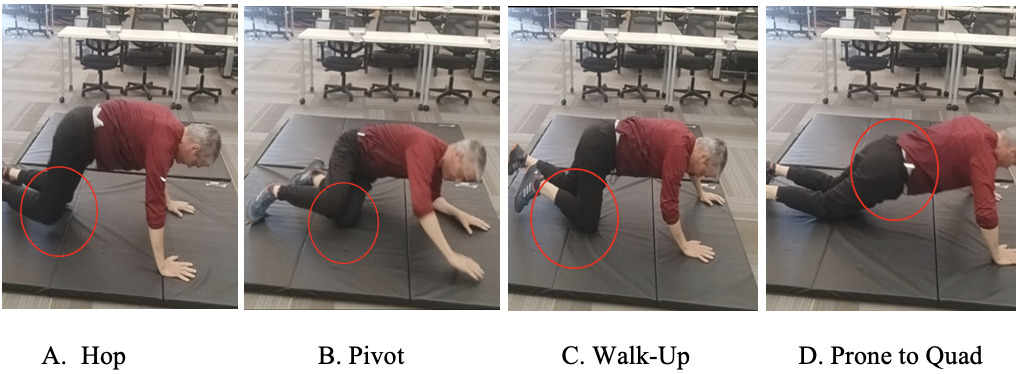
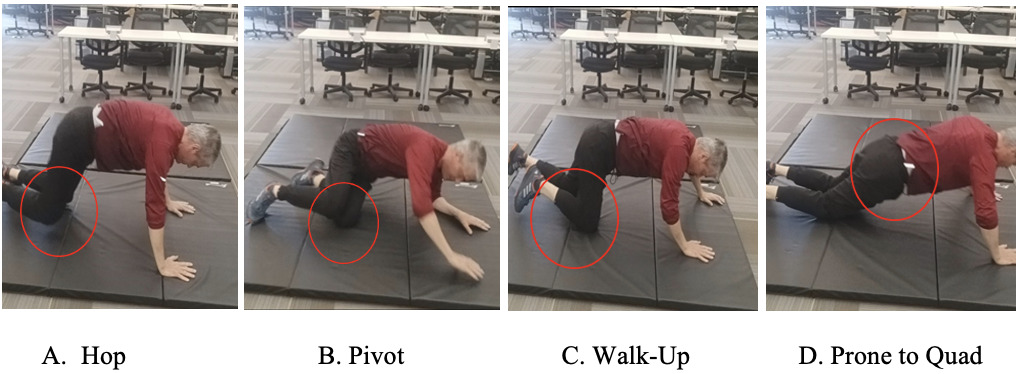
Three licensed physical therapists independently reviewed the video recordings to 1. Verify the number of successful rolls completed; and 2. Classify each participant’s rolling strategy into one of four categories: Hop, Pivot, Walk-up, and Prone to Quad (Figure 1). Consensus was reached through discussion when classifications differed.
Data Analysis
Descriptive statistics were used to describe participant characteristics and test results. An independent t test was first used to determine if mean differences between genders and total rolls, rolling strategies, upper and lower extremity strength and lower extremity and core endurance were statistically significant. Pearson product moment correlation analyses were also used to examine the relationships between 30RQ performance (number of total rolls and rolling strategy) and participant age, sex, activity levels, core endurance, upper and lower extremity muscle strength, BMI, and lower extremity endurance. For this study, a Pearson product moment correlation of < 0.40 was considered a weak correlation, a correlation of 0.40-0.69 was considered a moderate correlation, and a correlation of > 0.70 was considered a strong correlation.16
RESULTS
This study initially enrolled nineteen participants from a single academic institution. After excluding one participant who performed the 30RQ test incorrectly due to not having shoulders, hips and knees in a 90 degrees angle during quadruped prior to transitioning back to supine during all repetitions, eighteen participants (8 males, 10 females; mean age = 25.67 ± 2.1 years) completed all testing procedures. Most participants reported moderate activity levels based on self-assessment (Table 1). Male participants demonstrated a statistically significant higher total roll count in 30 seconds (19.38 vs 12.80 rolls; p < 0.01) when compared to female participants (Table 2). The pivot rolling strategy was the most used rolling strategy for both male and female participants with males demonstrating a statistically significant difference when compared to females (18.0 vs 7.9 reps; p < 0.01). Female participants were more likely to use the hop up (1.50 vs 1.13 reps), walk up (0.30 vs 0 reps), and a statistically significant increase in use of the prone to quadruped (3.10 vs 0.25 reps; p < 0.05) rolling strategies when compared to male participants (Table 2). Baseline strength measurements also revealed consistent statistically significant sex differences across all tested upper and lower extremity muscle groups (Tables 3 and 4). Sex differences for lower extremity endurance and core endurance measurements were not statistically different (Tables 3 and 4).
The prone to quadruped strategy showed distinct correlation patterns, including a moderate positive correlation with age (r = 0.669, p < 0.01) and moderate negative correlations with female sex (r = -0.483, p < 0.05), total roll count (r = -0.565, p < 0.05), and activity level (r = -0.486, p < 0.05). This strategy also demonstrated moderate negative correlations with multiple strength measures, including elbow extension (r = -0.566), shoulder abduction (r = -0.530), shoulder flexion (r = -0.496), hip abduction (r = -0.495), and hip flexion (r = -0.472; p < 0.05). The hop and walk-up strategies showed no significant correlations with any measured variables (Tables 5 and 6).
Overall performance on the 30RQ test, measured by total roll count, demonstrated strong positive correlations (r > 0.700, p < 0.01) with male sex (r = 0.770) and multiple strength measures. These strong correlations between male sex and strength measures were observed with hip strength measures including flexion (r = 0.785), abduction (r = 0.751), and extension (r = 0.726), as well as shoulder strength measures including flexion (r = 0.737), abduction (r = 0.759), horizontal abduction (r = 0.707), and horizontal adduction (r = 0.789). Moderate positive correlations were found for both male and female sex between total roll count and hip horizontal abduction strength (r = 0.575, p < 0.05), knee flexion (r = 0.685, p < 0.01) and extension strength (r = 0.671, p < 0.01), elbow extension strength (r = 0.655, p < 0.01), and 30-second Chair Stand Test performance (r = 0.495, p < 0.05). There were no statistically significant correlations between core endurance measures and total number of rolls or rolling strategies.
DISCUSSION
Primary Findings
The results of this study demonstrate several key findings regarding the 30RQ test. Analysis of rolling strategies revealed distinct patterns across the sample population. The pivot technique emerged as the predominant method, accounting for 79% of total rolls, followed by prone to quadruped (18%), hop (8%), and walk-up (1%). The pivot strategy demonstrated strong associations (r > 0.700) with male sex, increased total roll count, and upper extremity strength measures. Second, total roll performance strongly correlated with both upper and lower extremity strength measures, particularly in male participants. Third, distinct patterns emerged between rolling strategies and physical capabilities, with the pivot strategy associated with higher strength measures and the prone-to-quad strategy associated with female sex, lower strength measures and decreased activity levels.
Rolling Strategy Selection and Performance
The pivot strategy’s moderate correlations with hip and knee strength align with previous research linking increased muscle strength to rolling capability, particularly regarding core and hip strength.17 The sex differences observed in muscle strength, strategy selection and rolling performance may be attributed to established physiological differences, as male participants typically demonstrate increased muscle mass and type II muscle fibers.18 Neuromuscular coordination (movement order) and sequencing (movement timing) are also important to rolling.19 Muscular weakness is one reason why rolling capacity may be limited in participants, but future studies are needed to further assess specific neuromuscular coordination and sequencing during rolling for participants completing the 30RQ.19
The prone-to-quadruped strategy, used predominantly by participants with lower strength measures, may represent a compensatory movement pattern. This strategy’s moderate correlations with increased age, decreased activity level, and lower strength measures suggest it may be chosen when insufficient strength exists to perform the more demanding pivot technique. The limited use of hop and walk-up strategies likely reflects their biomechanical inefficiency for repeated performance, though their lack of correlation with any measured variables warrants further investigation.
Clinical Implications
These findings suggest that the 30RQ test may serve as a useful assessment tool for evaluating rolling ability and that rolling ability correlates with strength, sex, lower extremity endurance, and rolling strategy. The 30RQ test may provide clinicians with a way to assess rolling ability and strength and identify impairments that might be missed through traditional testing methods such as manual muscle testing.
The distribution of rolling strategies used during testing provides additional clinical insight beyond basic performance metrics. The current findings suggest that the proportion of pivot versus prone-to-quadruped strategies may serve as a qualitative indicator of strength and movement efficiency during rolling. A higher proportion of pivot strategy usage correlated with greater strength measures, while increased reliance on the prone-to-quadruped strategy may indicate areas requiring clinical attention. This pattern of strategy selection, combined with quantitative performance measures, offers clinicians a more comprehensive understanding of a patient’s strength and rolling abilities.
The vestibular demands of repeated rolling movements should be considered when interpreting test results. Some patients may demonstrate decreased performance due to vestibular processing rather than strength limitations, suggesting that clinicians should monitor for signs of vestibular involvement during testing. A modified version of this test, consisting of four repetitions (two complete circuits of rolling right and left to quadruped), might provide similar clinical insights while minimizing vestibular effects. This adaptation, like established strength tests like the Five Time Sit to Stand Test, could allow clinicians to assess both movement quality and strategy selection while timing the performance. Future studies should include a modified version of this test to minimize vestibular effects.
Limitations and Future Research
Several limitations should be considered when interpreting these results. The sample size was relatively small and homogeneous, potentially limiting generalizability. Additionally, the lack of EMG data prevents detailed understanding of muscle activation patterns during different rolling strategies. The 30-second duration of the test may introduce a vestibular component that could influence performance independent of strength capabilities. Some participants may experience dizziness or disorientation during repeated rolling, potentially masking their true strength capabilities and confounding test results.
Future research studies should address these limitations by using larger, more diverse sample populations and longitudinal studies to establish normative data and assess predictive validity. Future studies should also investigate using EMG analysis of muscle activation during different rolling strategies and investigate the test’s utility in athletic and clinical populations. Future studies should also develop standardized criteria for assessing and documenting rolling strategy selection.
The proportion of different strategies used during rolling may prove to be as clinically meaningful as the total number of rolls completed when assessing patients. Future research should explore whether strategy distribution patterns can serve as reliable indicators of strength and movement capability, potentially leading to the development of more refined clinical assessment tools.
CONCLUSION
The results of this study indicate that total roll performance was strongly correlated with increased upper and lower extremity strength measures, particularly in male participants. The pivot strategy demonstrated strong associations with male sex, increased total roll count, and increased upper extremity strength measures. The prone-to-quad strategy was associated with lower strength measures and decreased activity levels. The 30RQ may be a useful qualitative and/or quantitative test to clinically measure not only the task of rolling, but also strength patterns in the shoulder, hip, knee, elbow, as well as lower extremity endurance .The 30RQ does not relate significantly to core endurance as measured by the maximum duration plank test.
Conflict of Interest
The authors have no conflicts of interest to report.