INTRODUCTION
Anterior cruciate ligament reconstruction (ACLR) remains one of the most commonly performed procedures in sports medicine, with over two million reconstructions performed worldwide each year.1 Postoperative ACLR rehabilitation is a cornerstone of successful outcomes, influencing not only return-to-sport readiness but also the risk of ACL reinjury and long-term knee joint health.2,3 International guidelines emphasize structured, progressive ACLR rehabilitation with objective criteria guiding progression rather than fixed time frames.4,5 However, despite growing consensus, translation of these recommendations into daily practice remains inconsistent.6,7
A persistent challenge in rehabilitation sciences is bridging the “evidence-to-practice gap”.8,9 Even when clinicians are aware of guidelines, the uptake of evidence-based practice (EBP) depends on multiple factors including individual skills, organizational support, and cultural norms.10 Surveys across physiotherapy and allied health professions have consistently reported barriers to EBP such as limited time, insufficient access to databases, lack of confidence in appraising research, and workplace cultures that prioritize tradition or clinical intuition.11–13 Conversely, positive attitudes toward EBP are nearly universal, and clinicians acknowledge its value for improving patient care.12,14 This paradox highlights the complexity of moving beyond knowledge to consistent implementation.
The role of learning strategies is central in this process. Physiotherapists engage in a range of formal and informal methods to update their knowledge, from continuing education courses and workshops to peer discussions and independent searching of medical databases.15,16 Early-career clinicians often demonstrate greater familiarity with electronic databases and online learning tools, reflecting curricular shifts that have embedded EBP training into entry-level programs.12 Yet, confidence in critical appraisal remains variable, and without reinforcement, EBP skills can diminish over time.14 Exploring how clinicians choose, value, and apply different learning strategies provides insight into why guideline uptake varies, especially in specialized areas such as ACLR rehabilitation.7,17
Continuing education plays a pivotal role in maintaining and expanding EBP skills. Structured programs, mentorship opportunities, and communities of practice have been shown to enhance knowledge translation and clinical behavior change.16,18 However, access to high-quality continuing education remains uneven, and financial, organizational, and motivational factors often limit participation.14 In the context of ACLR rehabilitation, where practice evolves rapidly with new testing batteries and injury-prevention paradigms, the need for ongoing professional development is particularly acute.3,19,20
Another determinant of evidence integration is related to interprofessional communication. Rehabilitation after ACLR rarely involves a single professional; rather, it requires coordination among surgeons, physiotherapists, athletic trainers, and sometimes sports psychologists or coaches.21–23 Effective return to sport decisions rely on shared understanding of patient progress and the consistent use of outcome measures.6 However, communication is often ad hoc, relying on informal channels such as email or messaging applications, with limited structured training in interprofessional collaboration during physiotherapy education.24 Deficits in communication can fragment care, reduce adherence to objective criteria, and reinforce reliance on time-based decisions. Thus, understanding current communication strategies among physiotherapists is essential for identifying systemic barriers to evidence implementation.
The use of medical databases is another window into EBP integration. Accessing scientific literature is a prerequisite to applying guidelines and best practices, yet many physiotherapists report difficulty with search strategies, overload of information, or challenges interpreting complex research.12 Although PubMed and other databases are widely available, their uptake varies by generation, experience, and educational exposure.25 Evidence suggests that younger clinicians tend to use these resources more frequently, while more experienced practitioners rely on accumulated expertise or professional networks.12 Understanding these patterns in ACLR rehabilitation is critical, as the complexity of RTS decisions demands both updated knowledge and its effective communication to patients and colleagues.
Despite these recognized factors, little is known about how French physiotherapists navigate learning, communication, and EBP challenges in their daily management of patients undergoing ACLR rehabilitation. Previous surveys have primarily been conducted in North America or Northern Europe, and cultural as well as organizational differences may shape unique barriers and facilitators in France.12,14 Moreover, existing studies often focus on attitudes toward EBP in general rather than on rehabilitation practices for specific conditions such as ACLR. By targeting this clinical population, new insights can be generated into the everyday realities of physiotherapists tasked with guiding patients through demanding postoperative recovery processes.
Accordingly, the purpose of this exploratory survey was to describe learning strategies, interprofessional communication patterns, and medical database searching practices among French physiotherapists managing patients after ACLR, and to explore associations with professional characteristics. By mapping how clinicians learn, communicate, and integrate—or struggle to integrate—scientific evidence into practice, perceived barriers and enablers can be identified that may influence the adoption of evidence-based rehabilitation approaches after ACLR. Understanding these factors is a necessary step toward improving knowledge translation and, ultimately, outcomes for patients who have undergone ACLR.
METHODS
Study design
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional research26 and the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) where applicable.27 A nationwide, web-based, cross-sectional survey was conducted to investigate current rehabilitation practices among French physiotherapists treating patients after ACLR.
This study was reviewed by the Institutional Review Board of the Ramsay Healthcare Group (IORG0009085) and was approved. (reference: IRB00010835).
Participants and recruitment
Eligible participants were licensed physiotherapists currently practicing in France, regardless of their years of experience or clinical setting. Inclusion criteria were: (1) holding a valid professional registration number, (2) being involved in ACLR rehabilitation, and (3) providing consent to participate in the study. Exclusion criteria were physiotherapists not practicing at the time of the survey or those not involved in ACLR rehabilitation.
Recruitment was conducted via professional networks, mailing lists of physiotherapy associations, social media platforms (LinkedIn, Facebook professional groups), and utilized snowball sampling. Participation was voluntary, unpaid, and anonymous. The survey was accessible online for a 12-week period (February–May 2025).
Sample size and data quality
No a priori sample size calculation was performed, as the primary aim of this study was exploratory and descriptive. A precision-based estimation was nonetheless conducted using the standard single-proportion formula with finite-population correction (calculated in R, version 4.3.3; R Foundation for Statistical Computing, Vienna, Austria). Assuming a conservative prevalence of 50% and a 95% confidence level, approximately 400 responses would have been required to achieve a 5% margin of error for national representativeness. The final sample comprised 62 respondents, which precludes population-level generalization but can provide preliminary evidence of practice trends. Accordingly, the findings should be interpreted as hypothesis-generating and as a basis for subsequent large-scale investigations, rather than as definitive estimates of the French physiotherapy population.
Questionnaire development and validation
The survey instrument was developed based on existing literature on ACLR rehabilitation practices4,5,28,29 and refined through consultation with experts in sports physiotherapy and academic research. The questionnaire was piloted with five physiotherapists to ensure clarity and face validity, and minor modifications were implemented before dissemination.
The final questionnaire consisted of four sections:
-
Professional background – age, sex, years of practice, geographical region, and volume of patients who had undergone ACLR treated per year.
-
Education and learning methods – exposure to evidence-based practice, participation in continuing education, use of medical databases.
-
Clinical practice in ACLR rehabilitation – learning strategies, interprofessional communication methods, and use of medical databases related to rehabilitation decision-making.
-
Perceived barriers and facilitators – organizational constraints, access to equipment, patient expectations, and perceived barriers to interprofessional collaboration.
The questionnaire (Appendix 1) comprised 31 items: 15 closed-ended questions (including categorical yes/no items and Likert-type ordinal scales), six semi-closed questions combining predefined response options with a free-text field, and 16 open-ended questions allowing participants to elaborate on learning strategies, communication practices, and perceived barriers. A limited number of open-ended questions allowed participants to elaborate on perceived barriers. Barriers to continuing education and to evidence-based practice were assessed using closed-ended items and complementary open-ended questions, which were analyzed using descriptive summaries and thematic grouping (as described).
To ensure the scientific robustness of the instrument, the questionnaire underwent a stepwise development and validation process. Content validity was first established by a panel of three experts in sports physiotherapy and two researchers with expertise in survey design, who independently reviewed the items for clarity, relevance, and coverage of the construct domains.30 Minor wording changes were made following their recommendations.
Prior to dissemination, the questionnaire was pilot tested on a convenience sample of ten physiotherapists not included in the main study. Their feedback confirmed overall clarity, feasibility, and average completion time (< 10 minutes). No further modifications were deemed necessary.
Reproducibility was assessed using a test–retest procedure with the same pilot group (two administrations separated by a 2-week interval). Agreement for categorical items was evaluated using Cohen’s kappa coefficients, which ranged from 0.72 to 0.88, indicating substantial to almost perfect reliability.31 Internal consistency was examined for the Likert-type scales using Cronbach’s alpha, yielding a coefficient of 0.81, which exceeds the commonly accepted threshold of 0.70 for acceptable reliability.32
These findings suggest that the questionnaire demonstrated satisfactory validity, reproducibility, and internal consistency, ensuring its suitability for use in the present study.
Data collection
In accordance with the CHERRIES checklist, process metrics were reported where available. A total of 16,354 invitations to participate were disseminated through open professional networks. Because the survey was hosted on Google Forms, unique survey link views and questionnaire starts could not be reliably determined. Therefore, the view rate could not be calculated, and the participation rate was calculated using the number of submitted questionnaires divided by the number of disseminated invitations. The questionnaire was hosted on a secure online platform (Google Forms®). Participants accessed the survey through a dedicated hyperlink. No personal identifiers were collected. Each participant could submit the questionnaire only once. Consent was implied by voluntary completion of the survey after reading the introductory information page outlining study aims, anonymity, and confidentiality.
Variables and outcomes
The primary outcomes were self-reported learning strategies, communication practices, and bibliographic resource use among physiotherapists involved in ACLR rehabilitation. Exploratory outcomes included associations between these behaviors and professional characteristics such as age, years of experience, and ACLR caseload.
Data quality checks
To maximize data quality, the survey platform was configured to restrict each participant to a single submission. Automatic controls (unique response token and IP-based filters) prevented duplicate entries. Questionnaires with more than 20% missing responses were excluded from inferential analyses. However, partially completed questionnaires with at least 80% of core demographic and practice-related items completed were retained for descriptive summaries. Consistency checks were performed to identify illogical or contradictory responses, which were flagged and verified before inclusion.
Handling of missing data
No statistical imputation was applied. All analyses were performed on a complete case basis, with results reported on the sample size available for each variable. Missing data were described as frequencies and percentages in the Results section.
Data storage and confidentiality
All survey data were exported in comma-separated values (CSV) format and stored on a secure, password-protected institutional server. Files were encrypted and access was restricted to the core research team only. No personal identifiers (e.g., name, email, IP address) were collected at any stage. The study complied with the European Union General Data Protection Regulation (GDPR, Regulation EU 2016/679), and participants were informed that their responses would remain strictly confidential and used solely for research purposes.
Data Analysis
Demographic and professional characteristics were collected and analyzed as categorical variables. Age was grouped into four predefined categories (20–30, 31–40, 41–50, and >50 years). Professional experience was grouped into 0–5, 6–10, 10–15, and >15 years. Annual ACLR caseload was grouped into 0–10, 11–20, 21–30, and >30 patients.
Open-ended responses were analyzed using a simple descriptive content analysis. For all analyses, group definitions were predefined. Age was categorized as 20–30, 31–40, 41–50, and >50 years. Years of professional experience were categorized as 0–5, 6–10, 10–15, and >15 years. Annual ACLR caseload was categorized as 0–10, 11–20, 21–30, and >30 patients per year. Perceived encouragement for continuing education was recorded as a dichotomous variable (yes/no).
Two authors independently reviewed all free-text answers, grouped responses into inductive themes, and resolved discrepancies through discussion. Themes were summarized descriptively (i.e., number of respondents mentioning each theme), and illustrative anonymized examples were reported where relevant.
Statistical analysis
Data were analyzed using JASP (version 0.18.2, University of Amsterdam). All study variables were categorical and summarized as absolute frequencies and percentages. All variables are reported as absolute frequencies and percentages.
Comparisons between groups (e.g., age categories, years of professional experience, ACLR caseload, perception of continuing education) were conducted using Chi-square tests of independence. Odds ratios (ORs) were derived from 2×2 contingency tables associated with Chi-square tests of independence. No multivariable logistic regression models were performed, given the exploratory nature of the study, the modest sample size, and the limited number of events per subgroup, which could compromise model stability and interpretability. To quantify the strength of associations, OR with corresponding 95% confidence intervals (95% CI) were calculated. Statistical significance was defined as p < 0.05.
Given the modest sample size and the exploratory design, analyses were considered hypothesis-generating rather than confirmatory. Additional exploratory stratified analyses were also planned according to practice setting (private vs. institutional) and geographic region to evaluate whether observed trends were consistent across subgroups. All group comparisons reported in the results refer strictly to these predefined categories, which were used consistently across analyses, tables, and figures.
RESULTS
Participant characteristics
Participant characteristics are presented as frequencies and percentages for each predefined category (Table 1). A total of 62 questionnaires were submitted; based on 16,354 disseminated invitations, the participation rate was 0.38%. Because unique survey link views and questionnaire start were not available, the view rate and completion rate could not be calculated.
Overall, respondents were predominantly young and early-career clinicians (56.5% aged 20–30 years; 48.4% with ≤5 years’ experience), and most treated ≤20 patients who had undergone ACLR per year (Table 1).
Descriptive analysis
Learning methods and continuing education
Perceived encouragement for continuing education was evenly split (48.4% yes vs 51.6% no; Table 1). Lack of time was the most frequently cited barrier (32.3%), with cost and accessibility constraints reported less often (Table 1).
Interprofessional communication
Interprofessional communication relied primarily on email and instant messaging (59.7% and 56.5%, respectively), whereas other channels were reported less frequently).
Literature search and scientific resources
Scientific information resources most commonly included medical databases (77.4%) and specialized physiotherapy journals (54.8%), whereas other sources were used less frequently (Table 1). Confidence in bibliographic resources was varied, with 50.0% reporting being comfortable/very comfortable and 22.6% not comfortable (Table 1).
Barriers and perceived needs
Open-ended responses were synthesized into thematic summaries and were used to contextualize the quantitative findings. Consistent with the closed-ended responses, lack of time was the most frequently reported barrier to continuing education (32.3%), whereas financial and logistical constraints were less frequently cited (Table 1). Additional themes emerging from free-text responses included limited access to high-quality training opportunities and a perceived underestimation of the complexity of ACLR rehabilitation.
Inferential analysis
Influence of age
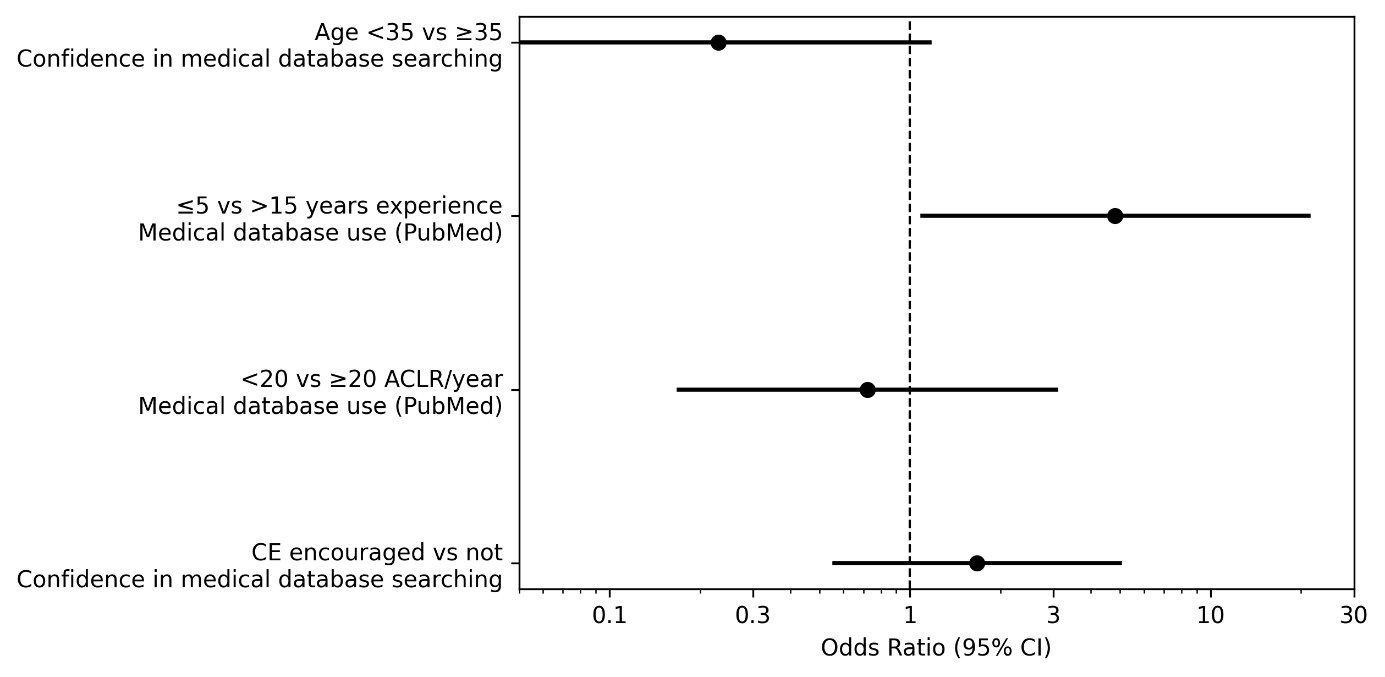
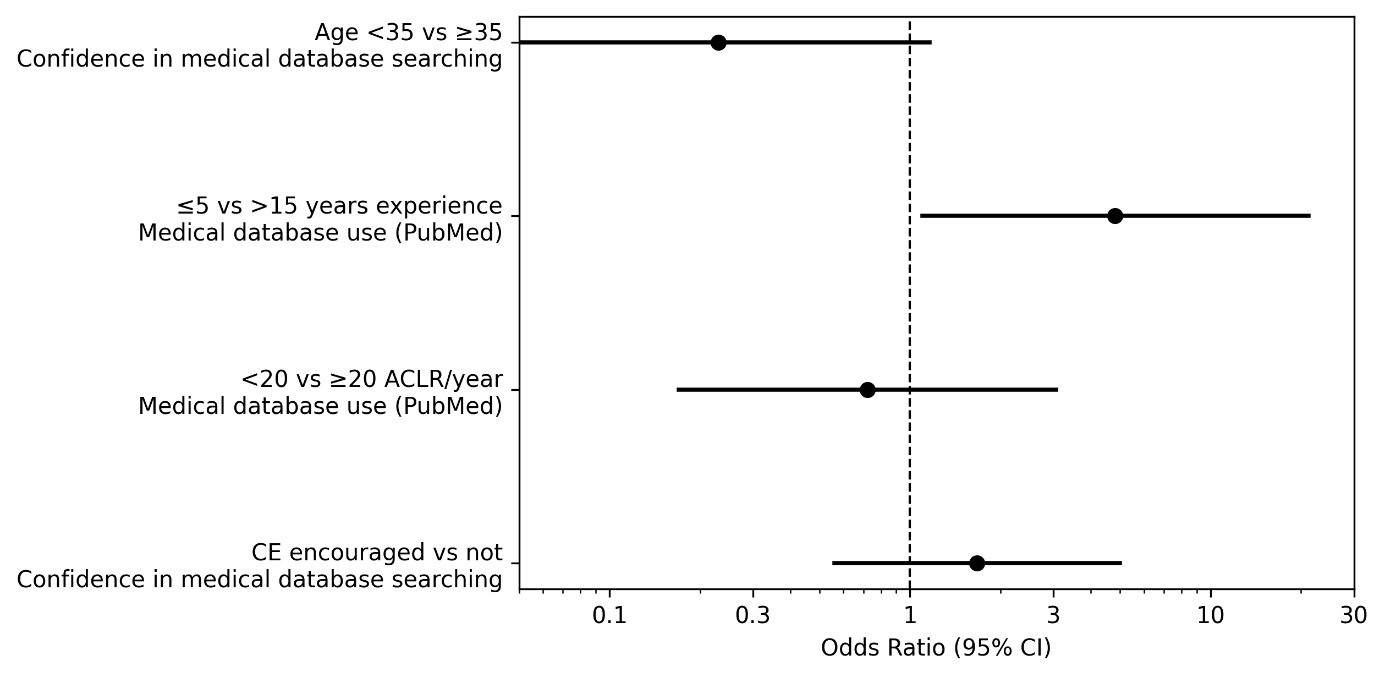
Physiotherapists younger than 35 years and those aged ≥35 years did not differ significantly in their confidence with bibliographic resources (Table 2). In this sample, physiotherapists aged <35 years tended to report lower confidence than physiotherapists aged ≥35 years (OR = 0.23 [0.05–1.16], p = 0.052), although this difference did not reach statistical significance (Figure 1).
Influence of years of experience
Professional experience was associated with the use of medical databases (Table 2). Physiotherapists with ≤5 years of practice showed higher odds of PubMed use compared with those with >15 years of experience (OR = 4.8 [1.1–21.2], p = 0.0012), while respondents with 6–15 years of experience showed values that fell between those observed in the ≤5 years and >15 years groups (Figure 1).
Influence of ACLR caseload
Annual ACLR caseload was not significantly associated with use of medical databases (Table 2). The odds of PubMed use did not differ between physiotherapists treating fewer than 20 versus ≥20 patients who have undergone ACLR treated per year (OR = 0.72 [0.17–3.06], p = 1.00) (Figure 1).
Perception of continuing education encouragement in the workplace
Perceived encouragement for continuing education in the workplace was not significantly associated with confidence in literature searching bibliographic research (Table 2). No significant difference was observed between respondents reporting sufficient versus insufficient encouragement (OR = 1.67 [0.56–4.99], p = 0.37) (Figure 1).
DISCUSSION
This exploratory survey set out to characterize how physiotherapists involved in ACLR rehabilitation in France learn, communicate, and engage with evidence-based resources. Three preliminary patterns emerge. First, self-reported engagement in searching for scientific information is variable: while a substantial proportion of respondents declared frequent use, many simultaneously reported difficulties in searching for and interpreting literature. Second, interprofessional communication appears largely informal and seldom supported by specific training. Third, years of professional experience appeared to influence literature searching practices, with higher reported PubMed use among clinicians with ≤5 years of practice compared with those with >15 years (OR = 4.8, 95% CI 1.1–21.2), albeit with imprecision due to small subgroup sizes. Importantly, the reported barriers provide context for these patterns, directly addressing the secondary aim and helping interpret the observed variability in continuing education engagement and literature searching. Together, these observations describe the professional context that may influence how evidence is sought, interpreted, and shared in rehabilitation after ACLR. Importantly, it was not explicitly assessed whether clinicians follow standardized rehabilitation protocols or clinical practice guidelines; therefore, the current findings should not be interpreted as measuring guideline adherence.
The mixed picture regarding use of medical databases is consistent with prior work suggesting that knowledge of evidence does not necessarily translate into systematic use of evidence in clinical decision-making.10,11 Surveys across physiotherapy and allied health consistently identify gaps in database literacy, critical appraisal, and confidence—despite overwhelmingly positive attitudes toward EBP.12,14 In the current sample, respondents frequently cited time constraints and difficulties interpreting scientific articles, echoing known barriers to EBP adoption such as workload, limited access to databases, and the complexity of research language.13,25 Educational interventions have been shown to improve discrete EBP skills (question-framing, search strategies, appraisal) and self-efficacy in students and early-career clinicians.15,16 However, in this sample, self-reported confidence and information-seeking patterns differed across experience groups, suggesting that institutional reinforcement (e.g., protected time, mentoring, and infrastructure) may be important to support consistent uptake and use of these competencies across career stages.33
The generational pattern that was observed—greater reliance on databases among early-career clinicians—likely reflects curricular evolution in physiotherapy, where EBP has become progressively embedded in entry-level training.34 Comparable effects have been reported internationally, with recent graduates displaying higher confidence in using databases and clinical guidelines than senior colleagues.8 Importantly, confidence is not synonymous with mastery. The data suggest that frequent users still identify interpretation as a sticking point. This resonates with prior findings that the translation step (from evidence retrieval to clinically actionable decisions) is the most challenging, especially when the available literature is complex, methodologically heterogeneous, or inconclusive—as is often the case in rehabilitation science.8
Interprofessional communication emerged as another critical dimension. Most respondents reported relying on email, calls, or messaging applications, and the majority indicated no formal training in interprofessional communication. This is noteworthy because ACLR rehabilitation frequently involves distributed teams—including surgeons, physiotherapists, athletic trainers, and sometimes psychologists—and safe progression hinges on timely, structured information exchange. Prior research in sports medicine and musculoskeletal rehabilitation emphasizes that return-to-sport decisions benefit from standardized criteria and shared language across stakeholders.6,21 Even though the utilized questionnaire did not measure specific use of objective tests or return-to-sport frameworks, the absence of structured communication training may contribute to variability in how evidence—when accessed—is conveyed and negotiated within teams. Literature on interprofessional education shows that explicit training in communication skills improves collaboration, reduces errors, and fosters more consistent adoption of evidence-based protocols.24
Practical barriers further shape these dynamics. Respondents highlighted time pressure and limited access to specialized equipment as recurrent obstacles. Prior studies show that when objective assessment tools (e.g., isokinetic testing, functional performance batteries) are scarce or impractical, clinicians default to heuristics and experience-based judgments.35 Again, the study did not directly measure testing practices; however, the combination of limited time, varied confidence in literature use, and the common use of informal communication channels suggests a plausible context in which evidence may be inconsistently integrated into clinical decision-making. Implementation science consistently demonstrates that multi-level strategies—combining training, feedback, workflow redesign, and leadership support—are required for sustainable change.36
The observed pattern invites two interpretive nuances. First, the early-career advantage in database use may coexist with lower self-confidence in interpretation, creating a paradox: younger clinicians retrieve evidence more often but may not always know how to critically integrate it. This can lead either to productive curiosity (seeking mentorship) or avoidance (relying only on abstracts or pre-digested content). Designing learning environments that pair younger clinicians with experienced colleagues—while simultaneously upskilling the latter in modern EBP workflows—could bridge this bidirectional gap. Evaluations of EBP mentoring and communities of practice suggest that such reciprocal arrangements are effective in raising collective standards.16,18 Second, improving communication quality may be as important as improving evidence access. When teams agree on shared outcomes, thresholds, and documentation standards—whether for progress reviews or surgical follow-ups—the costs of using evidence decrease, and the perceived return on investing in EBP skills increases.6,24
Finally, positioning these findings within ACLR rehabilitation is important. International consensus increasingly emphasizes structured, criteria-informed progression and transparent, team-based decision-making.2,3,37 The survey did not quantify clinicians’ direct use of such criteria; instead, it illuminates the learning and communication substrate upon which criteria-based approaches depend. In that sense, the results are complementary to guideline work: they identify where translational friction may reside (skills, time, tools, coordination) and were enabling conditions (continuing education opportunities, simplified resources, interprofessional pathways) may generate the greatest gains. Future research combining audits of actual rehabilitation practices with surveys of learning and communication would clarify how these domains interact and, crucially, which leverage points yield the most durable improvements in everyday care.
LIMITATIONS
This study has several limitations. First, the sample size was modest (n = 62) compared with the estimated target for adequate statistical power, which reduces the precision of effect estimates and limits the generalizability of the findings. This limitation is compounded by the low participation rate (0.38%), which increases the risk of non-response and self-selection bias, and suggests that respondents may not be representative of the broader population of French physiotherapists. Accordingly, p-values and OR should be interpreted cautiously and not as confirmatory evidence, but rather as hypothesis-generating signals, particularly when confidence intervals are wide. Therefore, survey should therefore be interpreted as exploratory and hypothesis-generating. Second, the questionnaire was specifically designed to assess learning strategies, interprofessional communication, and medical database searching practices among physiotherapists managing patients after ACLR —that may indirectly influence the adoption of evidence-based rehabilitation. Third, as with all self-reported surveys, responses may be affected by recall bias and social desirability bias, potentially leading to an overestimation of evidence-based behaviors. Finally, the cross-sectional design precludes any causal inference about the relationships observed between age, professional experience, and reported practices. Future studies with larger and more representative samples should consider multivariable logistic regression models to better account for potential confounding factors.
CONCLUSION
This exploratory survey provides preliminary insights into the professional environment of physiotherapists managing ACLR rehabilitation in France. The findings suggest a pattern of higher database use among clinicians with ≤5 years of practice compared with those with >15 years, while confidence in searching and interpreting scientific literature remained heterogeneous across respondents. Time constraints emerged as the most frequently cited barrier to continuing education, and organizational constraints (including limited consultation time and access to equipment) were recurrently reported as barriers to evidence-based practice. The absence of formal training in interprofessional communication also highlights a gap in current professional development.
Taken together, these results support strengthening continuing education opportunities, prioritizing training in database literacy and critical appraisal, and integrating structured interprofessional communication training within professional development. While these findings cannot be generalized due to the modest sample size, they emphasize key leverage points for improving knowledge translation in ACLR rehabilitation. Larger and representative studies are warranted to confirm these trends and to guide future interventions aimed at optimizing rehabilitation practices and patient outcomes.
Conflicts of interest
The authors declare that they have no conflicts of interest relevant to the content of this manuscript.