Introduction
Sports medicine physicians and physical therapists routinely evaluate and treat young athletes with low back pain (LBP). In this study, we define young athletes as children and adolescents (6–18 years) participating in organized sports. Approximately three-quarters of these young athletes present with extension-based low back pain (EBLBP), where the pain is greater with active lumbar extension than flexion.1 Between 32% and 64% of athletes with EBLBP have imaging evidence (radiograph, Magnetic Resonance Imaging (MRI), Single Photon Emission Computed Tomography (SPECT), or Computed Tomography (CT)) of spondylolysis or stress injury of the pars interarticularis.1–4 The etiology of pars injury is repetitive or acute lumbar spine loading in hyperextension and rotation during sports participation.4 Cumulative mechanical stress exceeds the body’s ability to dissipate the loads successfully.5–7 The L5 vertebra is most frequently affected (74.6%), followed by L4 (21.4%).8 Radiographs are often insufficient in identifying early spondylolysis.2,9 Consequently, clinicians order additional imaging such as MRI SPECT, and CT, which adds to the financial cost and, in the case of SPECT and CT, exposes the athlete to ionizing radiation, increasing the risk of cancer.10–13 CT scans are sometimes used to evaluate and monitor bony healing, although their routine use remains debated.14,15 There are conflicting opinions regarding the appropriate use of imaging to evaluate LBP in young athletes.9,14,16
There is mounting evidence that the pain associated with EBLBP may not correlate closely with structural imaging findings.7,17 In some cases, athletes continue to experience nociceptive pain despite radiographic healing, while others have complete resolution of symptoms despite a non-union of the fracture.6 Similar patterns have been reported more broadly in LBP populations, where structural abnormalities on MRI are frequently observed in asymptomatic individuals, indicating that imaging changes alone are poor predictors of pain or disability.18 Radiographic healing does not always translate into meaningful clinical improvement in pain and function.19 In a retrospective chart review, El Rassi and colleagues evaluated the effect of sports modification on clinical outcomes in children and adolescent athletes with symptomatic lumbar spondylolysis and found that bony healing did not predict favorable clinical outcomes in terms of pain relief, functional improvement, or return to sport.20 These findings suggest that the pars defect may not be the primary source of nociception, but rather a marker of extension overload, representing the mechanical stress experienced during participation in sports.
Approximately half of athletes with EBLBP have negative imaging for spondylolysis, yet their clinical presentation is identical to that of radiographically positive athletes.21,22 These extension-based imaging negative conditions may involve the posterior elements of the spine and have been referred to as hyperlordotic back pain, mechanical LBP, spondylogenic back pain, and lumbar facet syndrome.23 Few authors have acknowledged this subgroup of imaging-negative young athletes with EBLBP, and no treatment guidelines have been established. In one study, greater fatty infiltrate of the lumbar multifidus muscles (LMM) was associated with a longer time to return to play in young athletes with EBLBP, regardless of whether the athlete had positive or negative imaging⁵ These results suggest that less emphasis should be placed on bony healing and diagnostic imaging, and more on addressing LMM muscle atrophy and loss of motor control. Guidelines for adults with LBP without red flags (cauda equina syndrome, malignancy, fracture, and infection) recommend withholding radiographs during the first 6 weeks of management, but no such guidelines exist for the pediatric population.24 Existing expert-based recommendations, including Choosing Wisely statements and the American College of Radiology Appropriateness Criteria for LBP, similarly discourage routine early imaging in the absence of concerning clinical features and emphasize initial conservative management. Although these guidelines are not tailored specifically to young athletes with extension-based LBP, they provide a framework suggesting that frequent immediate radiographs and early advanced imaging in otherwise healthy children and adolescents may represent overutilization.
Management of spondylolysis in young athletes has historically focused on bony healing and preventing further structural injury. Traditional management strategies include restricting athletes from participating in practice or games, soft or rigid lumbar bracing, physical therapy, use of a transcutaneous bone stimulator, and, in rare cases, surgery.6,25–27 However, given the variability in both the timing and utilization of imaging modalities, as well as in management approaches, there is a clear need for evidence-based guidelines to standardize care and optimize outcomes in this athletic population.
The purpose of this study was to determine the imaging practices of sports medicine physicians who manage young athletes with EBLBP and provide evidence-informed recommendations.
Methods
An email invitation was sent to 2,185 physician members of a national sports medicine organization. Eligible recipients were board-certified sports medicine physicians with a primary specialty in either pediatrics, internal medicine, family medicine, physical medicine and rehabilitation, or emergency medicine who were currently in clinical practice. Email addresses were obtained from the organization’s membership database and used with permission for this study. Potential participants were not contacted individually prior to the study; the initial invitation and one reminder email were the only contacts.
The study protocol was determined to be minimal risk and received expedited approval from the Ithaca College Institutional Review Board prior to survey dissemination. The email, sent from the organization’s official email account, included a brief description of the study purpose, emphasized that participation was voluntary and anonymous, and contained a hyperlink to the 13-question online survey designed to identify sports medicine physicians’ imaging and treatment preferences for young athletes with EBLBP.
The survey instrument was developed through an iterative, multidisciplinary process. First, a discussion group comprised of sports medicine physicians, radiologists, physical therapists, and athletic trainers identified key domains of interest, including imaging preferences, nonoperative management strategies, and practice characteristics relevant to extension-based low back pain in young athletes. Draft items were generated to cover these domains and refined during group meetings to improve clarity, reduce redundancy, and ensure that questions reflected realistic clinical scenarios. Once consensus was reached, three independent board-certified sports medicine physicians who were not involved in item generation reviewed the survey for content and face validity. Based on their feedback, minor wording changes were made to improve readability; no items were added or removed. The final survey was organized into three sections: (1) imaging preferences, (2) treatment and management preferences, and (3) respondent characteristics, including practice setting and percentage of sports medicine caseload. The full survey instrument is provided in Appendix A.
Descriptive statistics were used to summarize survey responses, including frequencies and percentages for categorical variables related to imaging and treatment preferences. These analyses provided an overview of physician practices and decision-making patterns.
In addition to the primary descriptive analyses of imaging practices, exploratory subgroup analyses were conducted to evaluate whether physicians’ imaging decisions differed by selected practice characteristics. Physician characteristics were derived from three survey items:
Q11 (“What percentage of your practice is spent in sports medicine?”), Q12 (“Which practice setting best characterizes your practice?”), and Q13 (“How many years have you been practicing sports medicine since your residency / fellowship?”). For Q11, responses were categorized as 0–25%, 26–50%, 51–75%, and 76–100% sports medicine. For Q12, practice setting was analyzed using the original response categories (orthopaedic office, multi-specialty group, hospital-based practice, private sports medicine practice, residency program, student health, urgent care center, and other). For Q13, years of experience were grouped as 0–5, 6–10, 11–15, and >15 years in sports medicine.
Imaging-related outcomes for subgroup comparison were selected from the main survey items as those most directly reflecting imaging decision-making: Q1 (frequency of radiograph use at the initial visit for extension-based low back pain), Q2 (timing of radiographs if not obtained at the initial visit), Q6 (timing of advanced imaging such as MRI, CT, or nuclear imaging), and Q7 (type of advanced imaging modality typically ordered to diagnose spondylolysis).
For each combination of physician characteristic (Q11, Q12, Q13) and imaging outcome (Q1, Q2, Q6, Q7), contingency tables were constructed and chi-square tests of independence were used to assess whether the distribution of imaging responses differed across categories of the physician characteristic. Analyses used only respondents with non-missing data for the two variables in each comparison. Because these subgroup comparisons were exploratory and involved many statistical tests, there were no adjustments made for multiple comparisons. This raises the likelihood of chance findings, so p-values are presented descriptively to indicate possible patterns rather than firm conclusions. Analyses were performed in Python using standard libraries, with α = 0.05.
Results
Out of 2,185 sports medicine physicians presented with the survey, 397 completed the survey, resulting in an 18% response rate.
Physician Imaging Practices
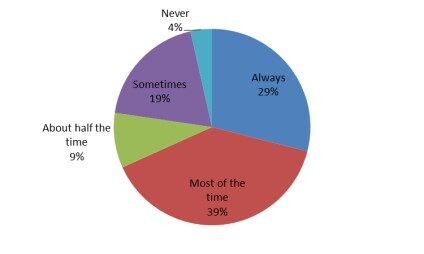
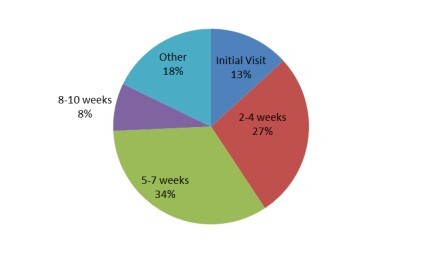
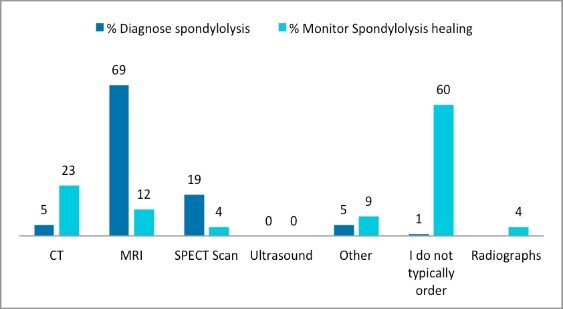
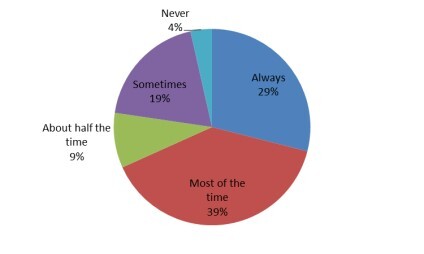
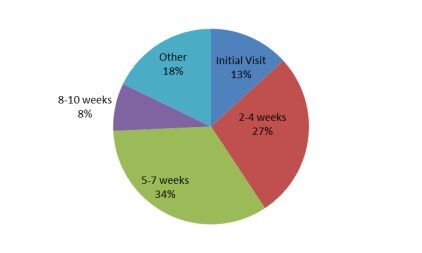
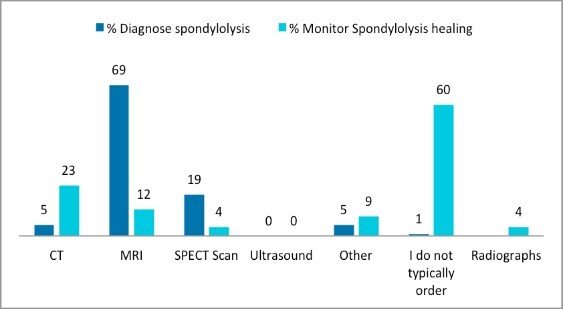
Almost three-quarters of sports medicine physician respondents, 271 (68%), reported that they always or most of the time order radiographs on the first visit (Figure 1). The most common views were anterior-posterior, reported by 382 (96.2%) respondents, lateral, reported by 376 (94.7%) respondents, and oblique, reported by 243 (61.2%) respondents. The reason for ordering radiographs was ranked in the following order: spondylolysis 223 (56.2%), spondylolisthesis 82 (20.7%), other 37 (9.3%), cancer 23 (5.8%), non-pars fracture 19 (4.8%), infection 5 (1.3%), scoliosis 4 (1.0%), and spondyloarthropathies 4 (1.0%). When asked when they typically order advanced imaging, 52 (13.1%) respondents indicated that they do so at the first visit (Figure 2), and 108 (27.2%) reported ordering advanced imaging within 4 weeks. The advanced imaging modality of choice was MRI 275 (69.3%), followed by SPECT 76 (19.2%), CT 20 (5.0%), and other 21 (5.3%) (Figure 3). Five respondents (1.3%) reported that they do not order advanced imaging. To monitor bony healing in cases of a confirmed spondylolysis, 239 (60.2%) respondents stated that they do not typically order additional imaging; among those who do, 91 (22.9%) reported using CT, 47 (11.8%) used MRI, 35 (8.9%) radiographs, 16 (4.0%) other modalities, 15 (3.8%) SPECT, and 239 (60.2%) stated they did not typically order additional imaging to monitor bony healing (Figure 3).
Subgroup Analyses of Physician Imaging Practices
Exploratory subgroup analyses were performed to evaluate whether imaging practices differed by percentage of sports medicine in the practice (Q11), practice setting (Q12), and years in sports medicine practice (Q13). Initial radiograph use and the timing of deferred radiographs were largely similar across sports-medicine caseload groups but varied by practice setting and years in practice. In contrast, the timing and modality of advanced imaging showed greater variability across all three subgroup dimensions.
When physicians were grouped by the percentage of their practice devoted to sports medicine, the proportion reporting that they “always” or “most of the time” obtained radiographs at the first visit did not differ significantly across groups (p = 0.36). Similarly, among visits without radiographs at the initial visit, the timing of subsequent radiographs was comparable across groups (p = 0.70). In contrast, the timing of advanced imaging (e.g., MRI, CT, or nuclear imaging) and the choice of advanced imaging modality varied by sports caseload: physicians whose practices were 76-100% sports medicine were most likely to obtain advanced imaging and to do so earlier, and MRI was the preferred modality in every case load group, with SPECT use varying across sports medicine caseload groups. (p=0.024 for timing; p=0.015 for modality) (Table 1).
Practice setting was more clearly associated with imaging behavior. The frequency with which radiographs were ordered at the initial visit differed significantly by practice setting (p < 0.001), with radiographs most commonly obtained at first visit in orthopedic offices and private sports medicine practices and less often in hospital-based and residency program settings. The timing of advanced imaging (p < 0.001) and the preferred advanced imaging modality for diagnosing spondylolysis (p = 0.004) also varied by practice setting: across all settings, MRI was the predominant modality, but orthopedic offices and private sports medicine practices more often reported using SPECT in addition to MRI, whereas hospital-based practices relied more heavily on MRI alone. By contrast, the timing of radiographs when not obtained at the first visit did not differ meaningfully across settings (p = 0) (Table 2).
Years in sports medicine practice showed a similar pattern. The proportion of physicians who always or most of the time ordered radiographs at the initial visit varied significantly by experience level (p = 0.014), with the highest rates among those in their first 5 years of practice and somewhat lower rates among those with more than 15 years of experience. The choice of advanced imaging modality also differed by years in practice (p = 0.002): MRI was the predominant modality across all experience groups, but less-experienced physicians (0–5 years) relied most heavily on MRI alone, whereas more-experienced physicians (>15 years) were relatively more likely to use SPECT in addition to MRI. However, there were no significant differences by experience in the timing of radiographs when deferred beyond the initial visit (p = 0.39) or in the timing of advanced imaging (p = 0.89) (Table 3).
Treatment Preferences of Sports Medicine Physicians
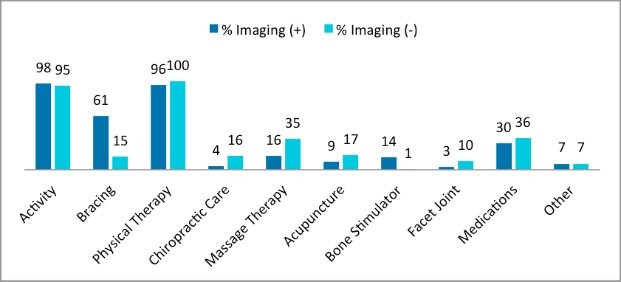
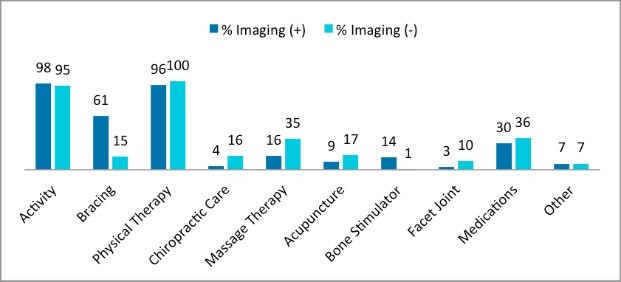
The most common treatment options for imaging-positive patients (patients with a spondylolysis), included activity modification 390 (98.2%), physical therapy 381 (96%), bracing 241 (60.7%), medications 121 (30.5%), massage therapy 63 (15.8%), bone stimulator 56 (14.1%), acupuncture 37 (9.3%), other 26 (6.6%), chiropractic 16 (4%), and facet injections 13 (3.3%) (Figure 4). Treatment options for imaging negative patients (patients without spondylolysis) included physical therapy 396 (99.8%), activity modification 377 (95%), medication 143 (36.0%), massage therapy 138 (34.8%), acupuncture 67 (16.9%), chiropractic 65 (16.4%), bracing 61 (15.4%), facet joint injections 39 (9.9%), other treatments 27 (6.8%), and bone stimulator 4 (1%) (Figure 4).
Discussion
Although evidence-based guidelines for adults with LBP without red flags (cauda equina syndrome, malignancy, fracture, and infection) advise withholding radiographic imaging during the first six weeks of management,24 no formal pediatric-specific guidelines have been established for the evaluation of LBP in young athletes. As a result, imaging practices in this population vary widely, often depending on provider preference and clinical suspicion. Based on the results of this survey, it is likely that an athlete presenting with LBP to a primary care sports medicine physician will undergo radiographic imaging on the first visit. When viewed in the context of adult low back pain guidelines, which discourage routine early imaging when red-flag features are absent, this pattern suggests that radiographs may be overused at the initial visit for young athletes with EBLBP, although this conclusion is based on extrapolating from adult rather than youth-specific guidelines. This practice is not unexpected as it likely reflects patient and parent expectations, the clinical emphasis on early identification of pars defects, and physicians’ concerns about serious pathology and the potential litigation.
Clinical Decision-Making - Imaging
Twenty-three physicians (5.8%) chose cancer as the primary reason for ordering radiographs. However, primary or metastatic cancer, as the cause of LBP in most populations is rare28 and radiographs are not highly sensitive or specific in the detection of spinal malignancies.29 In a study conducted by Deyo and Diehl, the prevalence of cancer-related back pain among 1,975 consecutive primary care patients with low back pain was .66%.28 After conducting this survey, the authors did an extensive review of 4,756 imaging records of individuals <21 years old referred to the radiology department at Cayuga Medical Center, Ithaca, NY, with LBP. Of the 4,756 cases, no cancers were identified on radiographs.
In a retrospective review of fifty adolescents with L5 spondylolysis, there was no difference in sensitivity or specificity whether an oblique view was included, as evaluated by four pediatric neurosurgeons.30 This finding was supported by Miller’s retrospective study of 194 patients that found no significant difference between two-view and four-view radiographs for diagnosis of spondylolysis.14 The majority of spondylolysis occurs at the L4 and L5, but the oblique view is better at imaging pars defects in the upper lumbar spine.31 Despite evidence demonstrating no difference in the sensitivity and specificity when including the oblique view,30 61.21% of sport medicine physicians surveyed stated that they typically include the oblique view when ordering radiographs.
The majority of the sports medicine physicians surveyed were most concerned with the presence of spondylolysis and spondylolisthesis. Lundine and colleagues found that nonoperative management or “watchful waiting” of the symptomatic young athlete (<18yrs old) with a high-grade spondylolisthesis is safe and does not lead to significant problems.32 They concluded that delayed surgical intervention in high-grade spondylolisthesis does not result in worse outcomes.32 Even if the athlete has an underlying high-grade spondylolisthesis, participating in conservative care did not result in a worse outcome.
Athletes with LBP are also likely to undergo advanced imaging (MRI, SPECT, or CT) within the first four weeks of evaluation. These imaging modalities contribute to increased healthcare costs and, in the case of SPECT and CT, expose the athlete to ionizing radiation, which carries a significantly higher risk of cancer for children compared to adults, estimated to be nearly tenfold greater.33 The risk of radiation-induced cancer is higher for girls than boys and is greatest with abdomen/pelvis CT scans.11 Although there are circumstances in which CT or SPECT may be justified—for example, when MRI is inconclusive (e.g., limited image quality or subtle findings), or unavailable, and there remains high clinical suspicion for a pars fracture that would influence management—these situations should represent targeted, problem-solving use rather than routine practice. The concern of the authors is therefore not that all CT/SPECT use is inappropriate, but that the relatively frequent, early use of ionizing imaging suggested by the results of this survey may reflect reflexive rather than selective use. While MRI is considered the gold standard for diagnosing spondylolysis due to its high sensitivity and lack of ionizing radiation exposure, challenges remain, including high cost, insurance coverage, limited access, and variability in imaging quality across institutions.34
The exploratory subgroup analyses suggest that potential overutilization of imaging in young athletes is not evenly distributed but is shaped by contextual and physician factors. Across all subgroups, a high proportion of physicians reported obtaining radiographs at the initial visit, consistent with widespread first-line use of plain films despite limited pediatric-specific evidence to support routine early imaging. Differences by percentage of sports medicine in the practice were modest. By contrast, physicians practicing in student health, multi-specialty, and private sports medicine settings, as well as those with more years in sports medicine practice, were less likely to order radiographs at the first visit, whereas the timing of radiographs when they were deferred beyond the initial visit was largely similar across subgroups. Practice setting, years in sports medicine practice, and, to a lesser extent, sports-medicine caseload were also associated with substantial variation in both the timing and modality of advanced imaging. Hospital-based and training-oriented settings tended to delay advanced imaging, whereas student health, multi-specialty, and some private sports practices more often pursued earlier MRI or SPECT, and more-experienced clinicians were more likely to incorporate SPECT and CT in addition to MRI. These patterns suggest that use of both initial radiographs and advanced imaging is influenced more by local practice habits and clinician experience than by patient factors, emphasizing a need for clearer guidance on when and how to use imaging in this population.
In the authors’ view, imaging adds value to patient care only when it leads to a change in management that has the potential to improve clinical outcomes. Physicians must weigh the benefits against the risks, particularly when ordering imaging studies that involve ionizing radiation. The majority of LBP experienced by young individuals has an underlying musculoskeletal origin, with a very low incidence of infectious, neoplastic, and inflammatory conditions.35–37 Appropriate screening and physical examination by the physician and/or physical therapist will determine if imaging is warranted. Miller et al. recommend that advanced imaging should not be routinely performed in young athletes with LBP and should instead be deferred until the athlete fails an initial trial of conservative management, including activity modification and physical therapy.14
Clinical Decision Making - Treatment
In this survey, most physicians reported using some form of activity restriction as a core component of treatment for young athletes with EBLBP. For imaging-positive athletes with spondylolysis, 98.2% of respondents reported using activity modification, and 95% did so for imaging-negative athletes with EBLBP, indicating that most physicians restrict sports participation through relative rest and modified activity rather than complete cessation of daily function. Sports medicine physicians appear to focus on bony healing when imaging is positive, whereas they are more likely to recommend manual therapy when imaging is negative. Treatment for imaging-positive patients more frequently included bracing (61% vs. 5%) and bone stimulator use (14% vs. 1%). However, the literature does not support the use of bracing to enhance fracture healing or reduce motion at the site of the spondylolysis.38–40 Additionally, there is currently insufficient evidence to support or refute the efficacy of bone stimulators in treating imaging-positive EBLBP.41,42 Previous research regarding the quality of the lumbar multifidus muscle and return-to-play timelines highlights the importance of motor control and muscular function in recovery from EBLBP in young athletes.43 Respondents also reported higher referral for manual therapy in imaging-negative patients, with chiropractic care prescribed in 16% vs. 4% and massage therapy in 35% vs. 16% of cases, respectively.
Selhorst et al. conducted a pilot study evaluating an alternative model of care for adolescent athletes with EBLBP, comparing a physical therapy–first approach with a traditional biomedical model involving early imaging.34 The study included 16 athletes (mean age 15 ± 1.8 years; 50% female) and found that the PT-first group had a 88% reduction in advanced imaging use compared to the biomedical group. Clinical outcomes were similar between groups, with 100% of PT-first participants and 88% of biomedical group participants returning to full sport participation. These findings suggest that, in appropriately selected adolescent athletes, early conservative management may allow imaging to be reduced without compromising outcomes.
In the authors’ clinic, imaging is reserved for athletes presenting with red flag symptoms, while initial management emphasizes activity modification and physical therapy to reduce extension forces and improve lumbar motor control.
Limitations
A limitation of this study is the modest response rate (18.2%), which raises the possibility of non-response bias. Physicians who elected to complete the survey may have stronger views or more experience regarding imaging practices for young athletes with low back pain than non-respondents. As a result, the findings may not fully represent the views of all sports medicine physicians. However, the current response rate is comparable to those reported in prior physician survey studies,44,45 supporting the overall relevance of these findings. Persistently modest response rates are a common problem in physician survey research, largely driven by time pressures, survey fatigue, and competing clinical demands, so some degree of nonresponse bias cannot be excluded.
Conclusion
Sports medicine physicians commonly obtain radiographs at the initial visit to assess EBLBP in young athletes, and advanced imaging is frequently ordered within four weeks. MRI is the preferred advanced imaging modality to diagnose spondylolysis, and while most responders did not monitor healing radiographically, those who did used CT scans. While the overall management of imaging-positive and imaging-negative EBLBP is similar, physicians report a greater use of bracing and bone stimulators in imaging-positive cases, as well as more frequent use of manual therapy, joint manipulation, and injections in imaging-negative cases.
The variability in practice patterns observed in this survey emphasizes the need for evidence-informed imaging guidelines specifically tailored to young athletes with LBP, similar to existing adult LBP guidelines, to support more consistent and appropriate use of radiographs and advanced imaging in this population.
Conflict of interest
We affirm that we have no financial affiliation (including research funding) or involvement with any commercial organization that has a direct financial interest in any matter included in this manuscript. We declare that we have no conflict of interest related to the content of this work.