INTRODUCTION
Proximal hamstring tendinopathy (PHT) is a common diagnosis characterized by pain localized to the ischial tuberosity. It is typically exacerbated by maneuvers involving hip flexion and loading of the proximal hamstring, such as running and lunging, or compression of the tendon such as in prolonged sitting.1–7 PHT can affect athletes such as sprinters and runners, but also commonly affects non-athletes.8–10 PHT is thought to be a chronic, degenerative process influenced by mechanical overload and repetitive stretch of the tendon.4,9 While a diagnosis of PHT can be made clinically after thorough history and physical examination, additional imaging may be obtained to evaluate the integrity of the proximal hamstring and rule out other potential etiologies of pain.8,11,12 Hip radiographs may demonstrate cortical change at the ischial tuberosity with PHT, but soft tissue imaging such as magnetic resonance imaging (MRI) or diagnostic ultrasound (US) allows for closer investigation of the tendinous, myotendinous, and muscle belly structures.11–13 PHT exists along a continuum of tendon pathology, ranging from early reactive tendinopathy to tendon disrepair and degeneration, which ultimately may lead to partial-thickness tearing. Understanding where an individual lies on this continuum can help guide management, which in the majority of cases is non-operative. This includes activity modification, oral or topical medications, and progressive tendon loading with a goal of working up to eccentric exercises.1,3,8,10,14 For cases refractory to the above approach and/or those limited by pain, additional treatment options include image-guided peritendinous injections (e.g. corticosteroid and platelet-rich plasma [PRP]) and both radial pressure wave (RPW) and focused shockwave (FSW), classically referred to as extracorporeal shockwave treatment (ESWT), though there has been no consensus on optimal treatment to date.2,8,14–20 PRP can be an effective treatment for proximal hamstring tendinopathy, however if concurrent needle tenotomy is performed there is typically a period of immobilization and reduced load post-procedure for protection and to facilitate tendon healing.16,18,21,22 This post-procedural reduction in activity is often not desirable for athletes and active individuals. In contrast, shockwave treatment allows patients to continue their exercise and/or sport as pain allows.23,24
RPW and FSW involve the delivery of high-pressure sound waves that are propagated in tissues and have been proposed to lead to multiple cellular responses.25–28 Proposed mechanisms of action include increased cellular proliferation, angiogenesis, neovascularization and increased collagen synthesis, leading to tissue remodeling.29–34 It is important to distinguish between RPW and FSW as the physics of each waveform are fundamentally distinct and therefore should not be classified as one entity, and though a detailed review of RPW and FSW is beyond the scope of this commentary, it remains important to understand the difference between RPW and FSW devices. Radial pressure waves have a greater superficial effect, with the maximum amount of energy delivered at the location where the applicator is placed on the skin and declining amounts of energy at greater depths, whereas focused shockwaves converge to deliver a maximal energy at a greater depth.24,35–37 RPW and FSW are often performed using a clinical focusing technique whereby the treatment is delivered over the area of maximal pain reported by the patient.23,24,38
Some previous studies demonstrate the efficacy of RPW and FSW for PHT,39–41 however, minimal guidance exists regarding optimal patient positioning during treatment. While this consideration may seem inconsequential compared to other parameters, positioning can influence tendon exposure and tissue depth and may impact adequate targeting of the proximal hamstring. Multiple studies have described utilizing clinical focusing technique for shockwave delivery, but not all describe the exact positioning during treatment.1,2,26,42 Therefore, the purpose of this narrative review and clinical commentary is to report what has been described for patient positioning during treatment of PHT with RPW or FSW and propose an alternative side lying approach.
METHODS
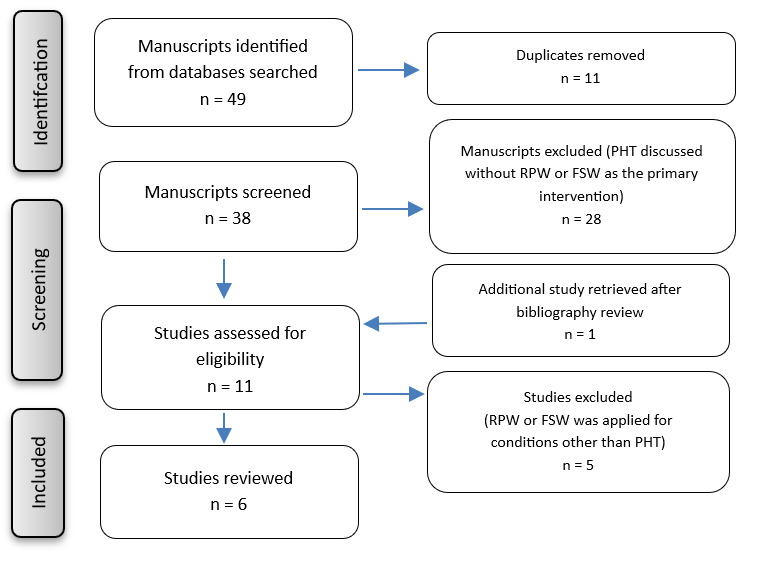
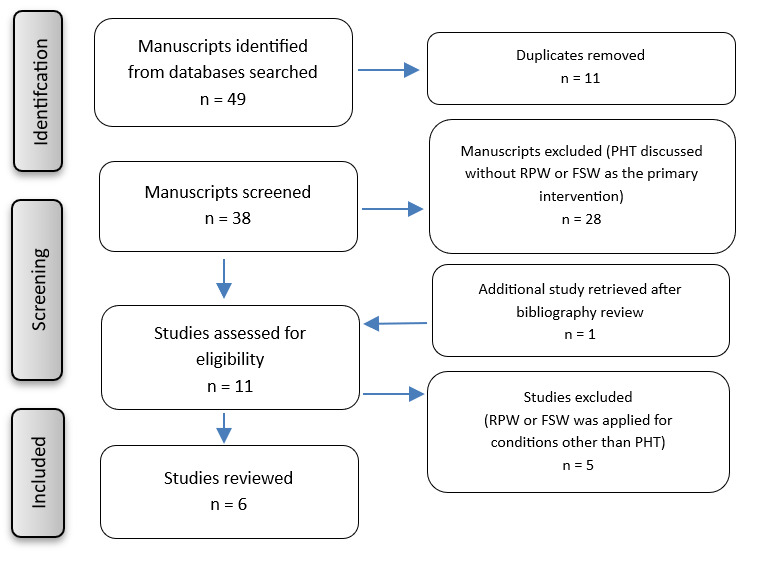
A search was conducted of MEDLINE/PubMed and EMBASE electronic databases for manuscripts published from January 2005 to January 2026. Key search terms included proximal hamstring tendinopathy, shockwave therapy, extracorporeal shockwave treatment, radial pressure wave, hamstring tendinosis, hamstring tendinitis, and hamstring pain. Studies were included if they evaluated RPW or FSW for the treatment of PHT. Studies were excluded if RPW or FSW was applied for conditions other than PHT, or if PHT was discussed without RPW or FSW as the primary intervention. All retrieved manuscripts (n=6) were screened for this review. Reference lists from the selected studies and review articles were further assessed for eligibility. Bibliographies were also reviewed for any relevant articles of interest. See Figure 1 for flow diagram for inclusion and exclusion of studies. Information from the six included studies were used to inform discussion of positioning during RPW or FSW for treatment of PHT and identify gaps in the literature.
RESULTS
Six manuscripts were included in the narrative review, two RCTs, two retrospective reviews, and two case reports (Appendix A). A total of 217 patients (145 female, 72 male) with PHT were treated with RPW and/or FSW in the identified manuscripts, although there may be some overlap in treated patients as the two retrospective reviews were published from the same institution. Patients included individuals diagnosed with PHT, ranging from professional athletes and runners to a para-swimmer. Four manuscripts used RPW to treat PHT, while two manuscripts treated patients with combined therapy with RPW and FSW.
Cacchio et al. studied 40 runners with chronic proximal hamstring tendinopathy in an RCT. The runners were diagnosed clinically with two out of three positive tests (Puranen-Orava test, fast hamstring-stretch test, and hamstring strength test) and a VAS pain score of greater than or equal to 4 at baseline evaluation. All patients had baseline MRI’s showing grade 2 or 3 tendinopathy per Khan et al. grading system for Achilles tendinopathy.43 Patients were randomized to a 1:1 ratio receiving RPW or traditional conservative treatment (TCT). RPW was applied weekly for four weeks, 2500 impulses were delivered at 4 bar and a frequency of 10 MHz. Clinical focusing technique was utilized with the placement of the applicator tip perpendicular to the area of maximal tenderness in a circumferential pattern. Patients were positioned supine, with the hip and knee flexed to 90 degrees respectively. Ice was recommended for the first four hours following treatment; patients were instructed to avoid NSAIDS and activities that exacerbated symptoms. Patients randomized to receive traditional conservative treatment (TCT) were recommended to rest and use NSAIDs for the first week, followed by physical therapy for two weeks and an exercise regimen for the remaining three weeks. Visual analog scale (VAS) and Nirschl phase rating scale (NPRS) were used as primary outcomes, and collected at baseline, 3, 6 and 12 months post-treatment. Secondary outcomes included the number of patients achieving a 50% reduction in VAS and patient-reported degree of recovery based on a Likert scale. Improvements were noted in VAS and NPRS at 3, 6 and 12 months post-treatment. At three months post treatment, 85% of patients treated with RPW had a 50% reduction in their VAS score compared to 10% in the TCT group and 80% of patients treated with RPW were able to return to their pre-injury level of sport activity.39
A second RCT published by Rich et al compared RPW and FSW to physiotherapy for management of PHT. Criteria for PHT included a three month or greater history of localized lower buttock pain with history of increased tendon load prior to the onset of symptoms and pain with at least three of four loading compression tests. One hundred patients were randomized to either receive four weekly sessions of RPW and FSW or six sessions of individualized physiotherapy. Radial and semifocused devices were used to administer interventions at 0, 1, 2 and 3 weeks; providing 2000 shocks at the maximum dose tolerated. Clinical focusing technique and patient positioning were not reported, nor were dosage details of EFD or MHz. Physiotherapy sessions occurred at 0, 1, 2, 3, 6, and 12 weeks.44 All patients received patient education and were able to continue normal activities, including exercise allowing for 4/10 pain with pain up to 2/10 in the 12-24 hours following. A global rating of change on a 7-point Likert scale and Victorian Institute of Sports Assessments-Hamstring (VISA-H) were used as primary outcomes and collected at baseline, 4, 12, 26, and 52 weeks with no significant differences noted between the shockwave group and physiotherapy group at any follow up interval. In secondary outcome measures, the shockwave group had higher self-reported satisfaction with treatment at 26 weeks and high satisfaction with the results of treatment at 4 and 26 weeks. Additionally, shockwave patients self-rated adherence to treatment was significantly higher for all follow up intervals.45
Mitchkash et al. retrospectively examined patient reported outcomes in a cohort of 94 runners. Lower extremity running-related injuries were included for review. Thirty-two of 94 runners were treated for PHT, who suffered from symptoms interfering with normal or typical training and inability to compete for greater than seven days. They received weekly treatments with RPW for four weeks. The number of impulses was not reported but the energy level ranged from 2-5 bar at a frequency of 12-15 MHz. Clinical focusing techniques were described to target the sites of pain during treatment. No other details were provided about patient positioning during treatment. Patients were encouraged to avoid icing and NSAIDS and continue physical therapy or a home exercise regimen. VISA-H was obtained at baseline, following ESWT and during follow-up visits. A 22-point improvement was used for the minimal clinically important difference (MCID). Sixty-nine percent of runners met the MCID.40
A second retrospective review was published by Yun et al. evaluating the use of combination therapy with FSW and RPW in a running cohort to treat PHT. PHT diagnosis was made based on history and physical examination. Sixty-three runners in total received either RPW in isolation or combination therapy with RPW and FSW. Forty received RPW and 23 received combined therapy with RPW and FSW for a minimum of four weekly treatments. Runners who did not improve with RPW alone were offered the option of combination therapy. RPW was administered at 2.5-5 bar, for 3000 impulses at a frequency of 15 MHz. For FSW, 1000 impulses at 0.12-0.5 mJ/mm2 were applied to the hamstring origin. Clinical focusing techniques were utilized to target the origin of the hamstring and additional regions as needed (e.g. myotendinous junction and muscle belly of affected muscle). For those receiving combination FSW and RPW, FSW was applied to the hamstring origin and RPW was applied to the myotendinous junction and muscle bellies (specific target was not reported). VISA-H was obtained at baseline, completion of treatment, and follow-up visits. All runners participated in concurrent physical therapy. Statistically significant improvements were noted in both groups, with 63% of patients who received RPW and 57% of patients who received combined FSW and RPW achieving MCID corresponding to a 22-point change in VISA-H. One patient who received radial shockwave went on to receive combined treatment and met the MCID thereafter. Outside of clinical focusing techniques, no other details were included about patient positioning during treatment.41
Two case reports using RPW for PTH have been published; a 25-year-old female ultramarathon runner and a 28-year-old elite female para swimmer. Treatment parameters are detailed in Appendix A. In both case reports, the treated athletes were able to successfully perform in their respective sport with reduced pain and improved function.46,47 Hayano et al. included a photograph of a RPW treatment utilizing a clinical focusing approach with the patient in a prone position.46
DISCUSSION
The current narrative review of the literature on the use of RPW and FSW in treating PHT reveals overall beneficial outcomes from the treatment. However, this review also demonstrates heterogeneity and lack of consensus on optimal treatment protocols related to the device being used, the use of RPW or FSW and/or combination therapy, number of impulses, energy level, peri-procedural considerations and patient positioning. This current review presents two reported patient positions in the literature – prone and supine with the hip and knee flexed.
Given the distinct physical properties of RPW and FSW devices, patient positioning may be expected to differentially influence energy transmission depending on the treatment used. FSW is characterized by convergence of acoustic energy at a defined focal zone located at a predetermined tissue depth based on the standoff employed. As such, patient positioning may influence the target of the focal zone relative to the proximal hamstring origin and may increase risk of off-target energy transmission to adjacent tissues if depth is not accurately estimated. In contrast, RPW exhibits maximal energy at the applicator tip, with progressive dissipation of energy as the acoustic waves travel in tissue. Therefore, there is potential that alterations in subcutaneous tissue positioning, tendon compression against the ischial tuberosity, and contact between the applicator head and skin could influence the energy transmission during RPW application. With utilization of clinical focusing techniques for both treatments, these differing physical properties may influence how effective the technique is based on the patient positioning. However, no current clinical evidence is available comparing the efficacy of RPW or FSW based on variations in patient positioning.
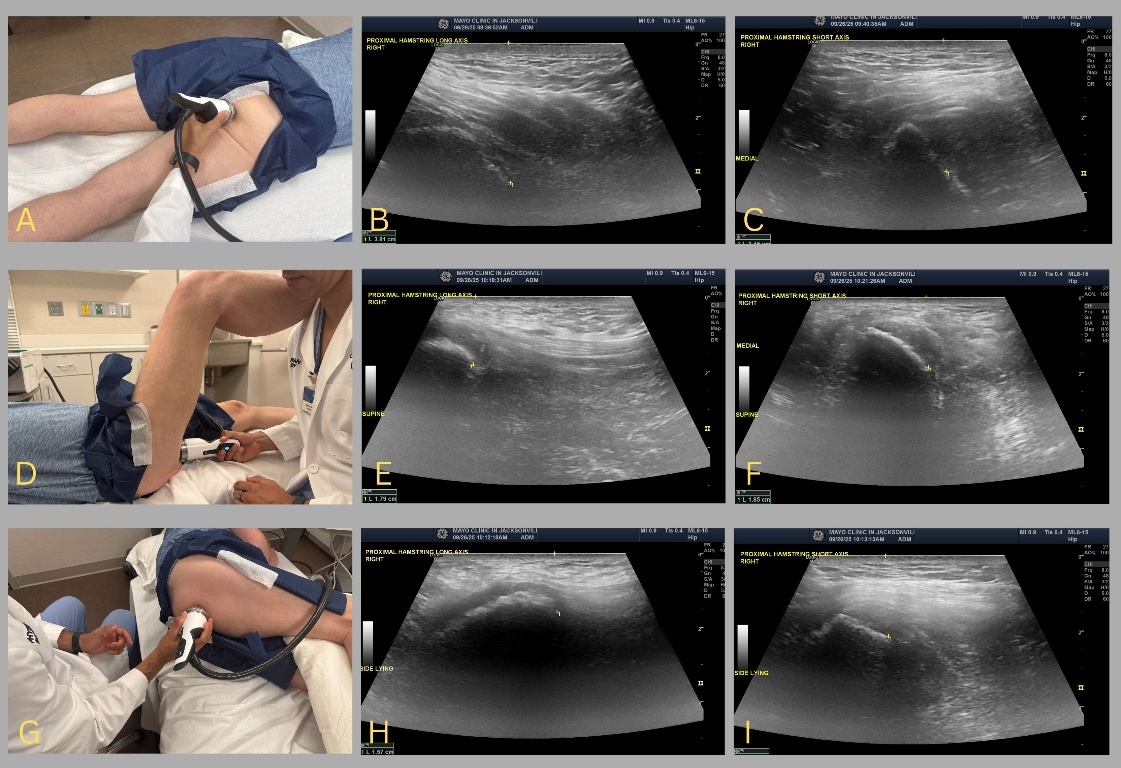
While clinical focusing has been described as a technique for both RPW and FSW, delivering treatment over the area of maximal pain reported by the patient, the position of a patient may alter how the sounds waves are transmitted and dissipated when targeting the proximal hamstring tendon. When in the prone position, the proximal hamstring is less exposed than in other positions, and, depending on the patient’s body habitus, adipose and subcutaneous tissue may act as a barrier to directly targeting the origin of the hamstring. Understanding the depth needed to adequately target the structure of interest is important as each device has a set focal zone of maximal energy which can be altered with different standoffs and/or the device used (e.g. RPW or FSW). A brief diagnostic musculoskeletal ultrasound to determine depth of the hamstring in the various different positions and can aid in localizing the proximal hamstring in relation to the skin surface (Figure 2). Additionally, if a shorter tip standoff is utilized to achieve a deeper focal zone, an inadvertent consequence may be that sound waves propagate to the anterior hip or adjacent neurovascular structures (e.g. pudendal nerve). The prone approach may be comfortable for most patients and is ergonomically efficient for the clinician administering the treatment. This approach may be more familiar to clinicians, as this position is commonly utilized for injection techniques.
__.jpeg)
While the supine with hip and knee flexed approach exposes the origin of the hamstring, this position may be hard to sustain for a patient and is less ergonomically efficient for the clinician (Figure 2D). However, since this position induces compression of the proximal hamstring against the ischial tuberosity, it may simulate a typical position that patients experience pain, increasing the utility of clinical focusing.
Based on the reported literature and sonographic depth depicted in Figure 2, when treating PHT with RPW or FSW, the author’s preferred approach involves having the patient side lying with the hip and knee flexed (Figure 2G). The degree of hip and knee flexion can vary based on patient comfort and body habitus, however there should be enough flexion to expose the proximal hamstring. A pillow is often utilized between the legs to improve patient comfort. While in this position, the patient and clinician’s comfort are maximized, and it does not require the patient to hold a sustained position. Additionally, the degree of hip and knee flexion can be easily adjusted as needed. This position also achieves the compression of the proximal hamstrings on the ischial tuberosity.
While patient and clinician comfort and exposure of the proximal hamstrings are important, it is not clear how variance in patient positioning affects outcomes, including patient-reported outcomes. No clinical study to date has reported outcomes utilizing this position, and no studies have utilized multiple patient positions as comparator groups. Therefore, future studies are needed to report on patient outcomes using the side lying approach in treating the proximal hamstrings, and a subsequent comparison study of patient positioning can be performed.
It is important to highlight the value of physical therapy and exercise in the management of PHT44 given that Rich et al. found no significant difference between RPW and FSW compared to individualized physiotherapy for treatment of PHT and both interventions were found to be beneficial.45 Additionally, Cacchio et al. instructed patients receiving RPW to avoid activities that increase pain, while other manuscripts mentioned physical therapy and continued home exercise regimens during post procedural guidance following RPW and FSW.39–41 PHT treatment recommendations most often include tendon loading exercise based on the patient presentation followed by progressive tendon loading with a goal of working up to eccentric exercises.44,48–52 Patients should be aware that pain while sitting may take longer to resolve and may lag behind return to function.53
This manuscript has several limitations. First, there is an overall paucity of literature on the use of RPW and FSW for PHT. Also, of the studies available, there is generally low-quality evidence, with only two RCTs and the remainder retrospective studies or case reports with heterogeneous outcome measures reported. Finally, there are no clinical studies with patient-reported outcomes utilizing the described preferred approach. While there is mention of the proposed benefits, it is difficult to know if and how this may influence patient outcomes.
Conclusion
Very few studies report the outcomes of shockwave application to treat PHT with only two prospective RCTs. Access to the PHT for clinical focusing of shockwave lends itself to multiple patient and provider positioning options and while clinical focusing techniques have been recommended for shockwave application,23,24 there is little described about patient positioning during treatment with no consensus on the optimal positioning for clinical efficacy. There remains a lack of standardized reporting for patient positioning and other parameters in studies utilizing RPW or FSW. In other areas of musculoskeletal medicine, consensus statements and professional societies have advocated for minimum reporting requirements when evaluating studies novel technologies such as orthobiologic injections,54 and this would likely be beneficial for shockwave studies as well. Future work should explore patient positioning and more prospective studies are needed to understand if patient positioning influences patient-reported outcomes.
Conflicts of Interest
The authors have nothing to disclose.
Corresponding author:
Jennifer R. Arthurs, APRN
Clinical Regenerative Medicine, Mayo Clinic
Jacksonville, Florida, USA
arthurs.jennifer@mayo.edu
Telephone (904) 956-3071
Fax (904) 953-2005