



Introduction
Hamstring Injuries (HSI) are a common time loss injury among elite-level athletes.1,2 Among National Collegiate Athletic Association (NCAA) championship sports, men’s football contributes the greatest proportion of hamstring strains at 35.3%, with 37.7% of these injuries resulting in time loss.3 Additionally, there is a high rate of recurrence for HSIs, with defensive backs, linebackers, running backs, tight ends, and wide receivers most at risk for reinjury.2 Among HSI’s, the biceps femoris is thought to account for the majority of HSIs with an occurrence rate between 65.8-83%.4,5 Semimembranosus injuries are estimated to account for 12-34.2% injuries and 5-31.6% of HSIs are thought to primarily involve the semitendinosus.4,5 Within hamstring injury literature, injury to the distal portion of the muscle or tendons of the hamstrings are considered less common, with even fewer accounts of distal semitendinosus tendon involvement.6 Due to the lack of research specific to semitendinosus tendon injury, management of tendon disruption or avulsion is controversial.6 The body of evidence is small, but it is estimated that nonoperative management of distal semitendinosus tendon disruption or avulsions have an injury recurrence rate of 42%.7 Additionally, return to play times, based on NFL data, is 12.8 weeks with non-operative management and 6.8 weeks with operative treatment.7 There are cases where individuals elected for conservative care for semitendinosus tendon avulsions required 10+ months of rehabilitation before full return to sport.8 Based on the timing of the upcoming season and the subject’s desire to minimize the risk for prolonged symptoms, he elected to proceed with operative treatment. Furthermore, distal avulsions of the semitendinosus from its pes anserinus insertion can cause recurrent symptoms if treated conservatively in multiple ways.7 The retracted semitendinosus stump can disrupt the length-tension relationship of the medial hamstrings and can cause aberrant hypertrophic scarring to occur in the posterior compartment of the thigh.7 Additionally, high-grade distal hamstring injuries are associated with enhanced scar formation, tendon hypertrophy, and soft tissue adhesions, often resulting in refractory pain and possible contributing to the low success rate of conservative care.7,9 This adhesive scarring process, paralleled with tendon hypertrophy, can result in fascial strictures within the popliteal region which can impair the athlete during full speed sprinting.9 Therefore, surgical intervention in the presence of distal semitendinosus tendon avulsion with retraction, instability, or displaying chronic symptoms from prior injury has emerged as a possible avenue for higher return to sport rates with less time loss for athletes.7,10,11
The surgical technique utilized with the athlete in this case report involves a single-incision tendon excision technique using a tendon striping tool. Among possible surgical techniques for this pathology, direct repair, anchor repair, tenotomy, and tenodesis have been suggested, however, the body of current evidence is small low-level regarding this injury.6,7,12–14 It is hypothesized that in the presence of distal semitendinosus tendon avulsions with retraction, repairing the tendon carries a high risk of re-rupture and/or ongoing pain at the repair site because of tension and scar tissue strictures, thus, tendon excision or tenodesis is suggested.9,15 In the excision procedure, the retracted semitendinosus tendon stump is identified using diagnostic MRI preoperatively, and subsequently identified via palpation or ultrasound guidance in the operating room.7,15,16 Following identification, the hypertrophied tendon stump is excised in its entirety.7,15,16
There is limited evidence in the literature regarding appropriate rehabilitation progression in terms of immediate post-op restrictions, exercise progression, and return to sport for patients who undergo a distal semitendinosus tendon excision. However, the tendon excision technique is gaining popularity as a potential solution for cases of tendon avulsion with retraction, instability, or chronic pain.11 Thus, there is a need for surgeons and physical therapists to generate a technique-specific rehabilitation guideline for these procedures. The purpose of this case report is to describe the rehabilitation program used for a collegiate American football player returning to sport after a distal semitendinosus excision.
Case Description
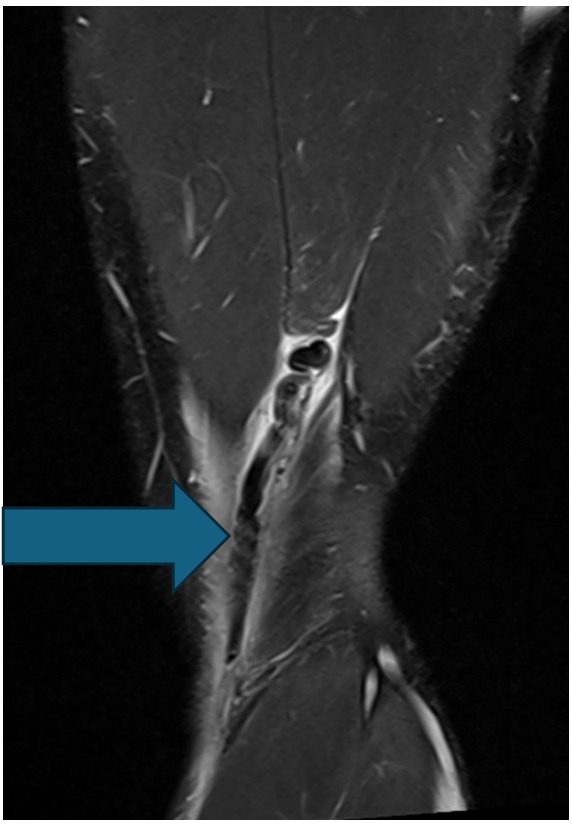
The subject was a 20-year-old male who was actively competing in collegiate American football within the Football Bowl Subdivision – the highest level of collegiate football in the United States. The subject originally sustained an injury to his distal posterior thigh on his nondominant left leg when performing resisted sprinting with a parachute attachment. While decelerating, the athlete slipped during the initial contact phase of his running gait, causing his knee to hyperextend and resulted in immediate posterior thigh pain. The athlete attempted to continue training during the session, however, ultimately discontinued participation due to high levels of pain at the distal posterior thigh. Upon evaluation by the athletic trainer, the athlete presented with pain upon resisted knee flexion and with a palpable defect at the posterior distal thigh. The athlete received an MRI shortly after the injury. The MRI revealed an avulsion of the distal semitendinosus tendon with 4 cm of cranial retraction (Figure 1). After all treatment options were discussed with the athlete and he was presented information regarding the high failure rates of conservative care and evidence of conservative cases with large variability in return to sport time, the athlete chose to proceed with the left distal semitendinosus tendon excision procedure for an expedited return to sport.
Timing of Outcome Assessments
Patient reported outcome measures were utilized to examine the subject at baseline after the procedure and then re-assessed at six and twelve weeks post operatively. Strength and functional performance measures were utilized at baseline on the uninvolved side, and as appropriate at six and twelve weeks postoperative to track readiness for returning to sport. Measurements were recorded until the athlete passed the determined return to sport battery and discharged from physical therapy. Satisfaction with the return to sport battery also included comparison to pre-injury metrics to determine final clearance.
Patient Reported Outcomes
The Functional Assessment Scale for Acute Hamstring Injuries (FASH) was used to quantify symptoms, severity, and functional disability of the subject. The FASH has excellent test-retest reliability (ICC = 0.9), internal consistency (Cronbach’s α = .98), and responsiveness (3.8 and 5.32 using baseline and pooled SDs).17–19 The FASH also possess established face validity, content validity, and construct validity in various athletic cohorts with hamstring injuries.17–19 Ceiling and floor effects were not found during the validation process for this questionnaire suggesting the FASH is an applicable tool for patients within the full severity range of hamstring injuries.17 The FASH contains ten question items including: seven questions utilizing a 0-10 numerical rating scale to quantify pain during various movements, and three questions using a categorical rating system on an incremental range of values to assess sports activity and demanding functional test. The highest score for the FASH is 100, representing normal/high level of physical function and ability.17 The minimum for the FASH is 0, indicative of complete disability following hamstring injury.17 Although the FASH has established reliability and validity, future work is needed to determine the minimal detectable change (MDC) and minimal clinically important difference (MDIC) for improved score interpretation and responsiveness.19
The Optimal Screening for Prediction of Referral and Outcome Yellow Flag (OSPRO-YF) tool is designed to assess negative mood, fear avoidance, and positive coping in individuals with musculoskeletal pain.20 It is a reliable and valid psychological assessment that evaluates three main domains including self-efficacy and acceptance, negative pain, and negative mood.20 Of the three domains, the OSPRO-YF generates scores for 11 psychological distress constructs based on patient responses. Scores that exceed the 75th percentile in negative pain coping or negative mood constructs or fall below the 25th percentile in self-efficacy and acceptance, indicate a possible “yellow flag” in those areas.21 The summary score of the OSPRO-YF counts the number of yellow flags identified. A greater number of yellow flags signifies elevated pain-associated distress, providing invaluable insights into the patient’s treatment response and need for psychologically informed intervention.21
The Single Alpha Numeric Evaluation (SANE) was used to assess the subject’s functional level compared to pre-injury levels. The SANE numeric scale ranges from 0-100 with 100 indicating normal/function at pre-injury level, and 0 indicating complete disability due to injury. The MCID for the SANE is 28.8.22 Though originally validated in the shoulder, the SANE has been established as a common patient reported outcome measure for HSIs and has shown moderate to strong positive correlations with other lower extremity outcome measures.23–27
Strength and Performance Measures
To objectively assess hamstring strength and performance, a series of tests were conducted to evaluate the patient’s physical readiness to run, practice, and subsequently return to sport. The performance testing battery included: isometric and eccentric strength measurements, countermovement jump testing on force plates and monitoring high-speed running tolerance with Global Positioning System (GPS) technology. Baseline testing began immediately post operatively with an isometric assessment of the uninvolved right side in a seated position with the feet off the ground, hip & knee flexed to 90-degrees (Figure 2), in prone with hip in neutral and knee flexed to 90-degrees (Figure 3), and in prone with hip in neutral and knee flexed to 15-degrees (Figure 3). The greater trochanter, lateral joint line, and lateral malleolus were used as anatomical landmarks to measure and set range of motion for each testing position. The line of pull for each testing position was perpendicular to the shin. Each isometric test was completed using a VALD Dynamo strain gauge (Vald Performance, Queensland, Australia). During each isometric test, the subject was instructed to produce as much force as fast as possible in each attempt and was given 30-second rest periods between attempts.
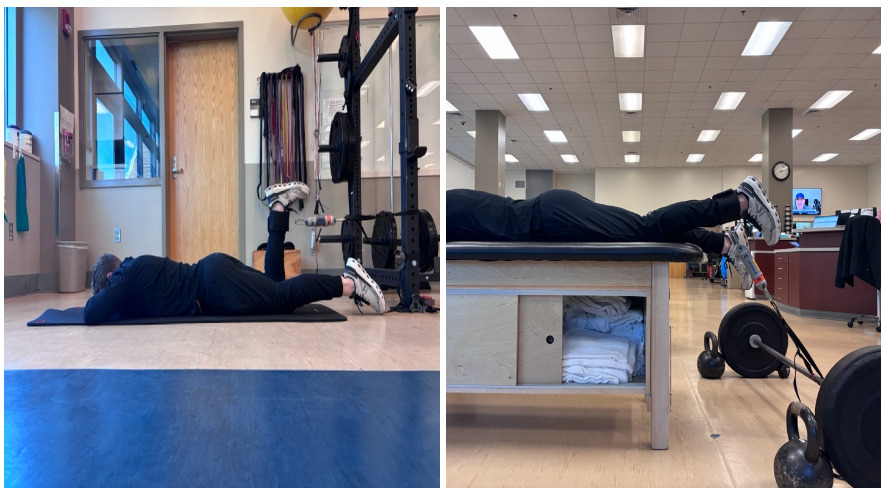
Once able, the subject initiated eccentric hamstring curl testing using the VALD NordBord (Vald Performance, Queensland, Australia) and hop testing using the VALD ForceDecks device (Vald Performance, Queensland, Australia). Eccentric hamstring curl and hop testing were formally assessed at six weeks to gauge readiness to begin running, and at twelve weeks as part of the return to sport battery. The athlete was instructed to complete eccentric hamstring strength and hop testing in accordance with recommendations for users from the VALD practitioners guide for each device.28–30 The NordBord eccentric hamstring curl test and ForceDecks countermovement jump test are depicted in Figures 4 and 5. Generally, Limb Symmetry Indices (LSI) close to 100% for strength and hop testing, and increased eccentric strength to bodyweight ratios are thought to correlate with a reduction in injury risk.31–33 Catapult GPS technology (Catapult Sports, Melbourne, Australia) was used to prescribe, monitor, and assess the athlete’s tolerance to high-speed running while returning to sport. Given the exponential increase in hamstring loading with high-speed running, and the reliability and validity of Catapult GPS technology to track athlete workload and performance during sport, the tool provided useful objective information.34–36



Surgical Procedure
In surgery, an oblique incision was made in accordance with the length of retraction observed on T2 axial and sagittal view MRI and over the palpable defect in the semitendinosus tendon. Care was taken to identify and preserve the gracilis tendon and saphenous nerve. Subcutaneous tissue and fascia were identified and incised, and no other notable pathologies were observed.
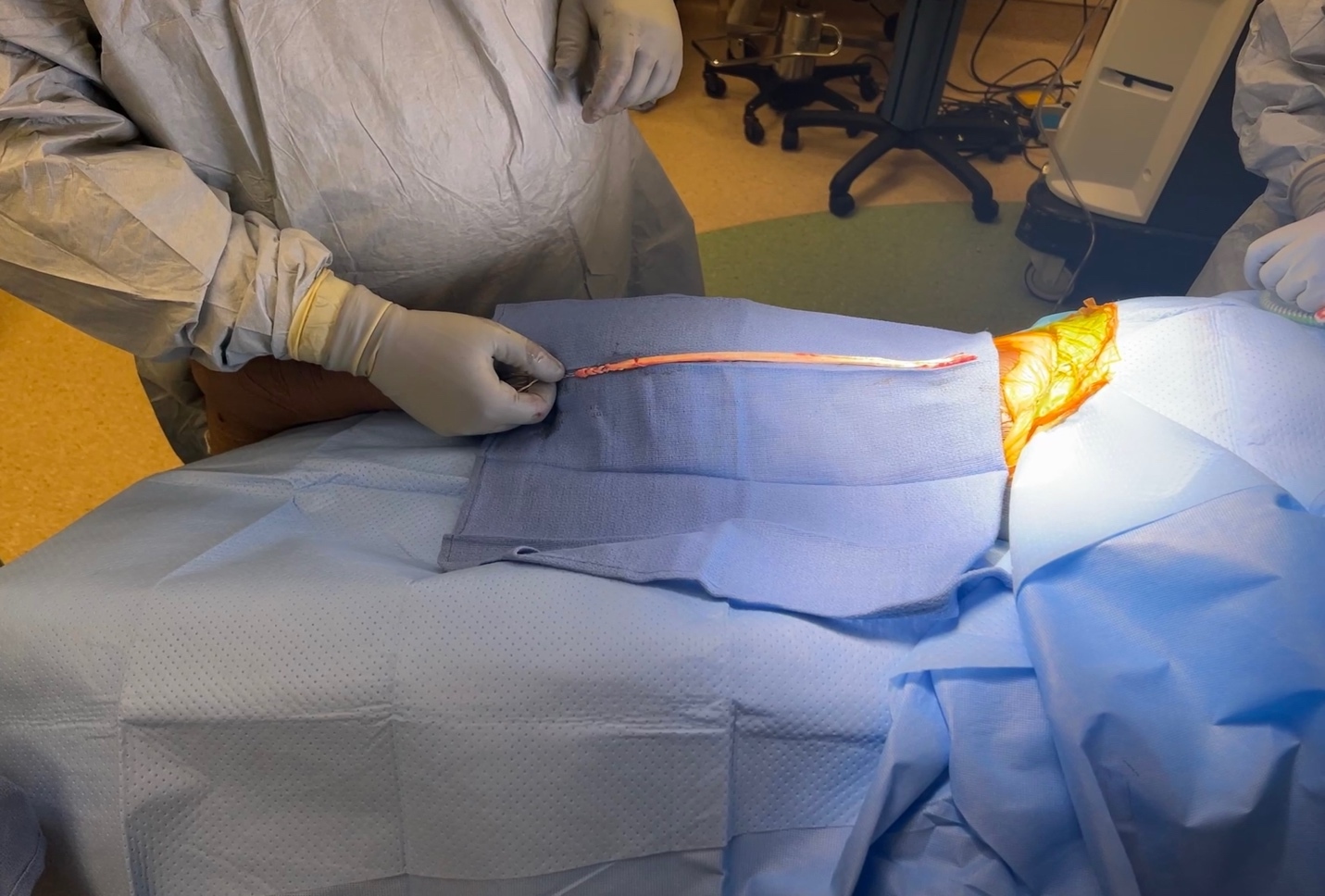
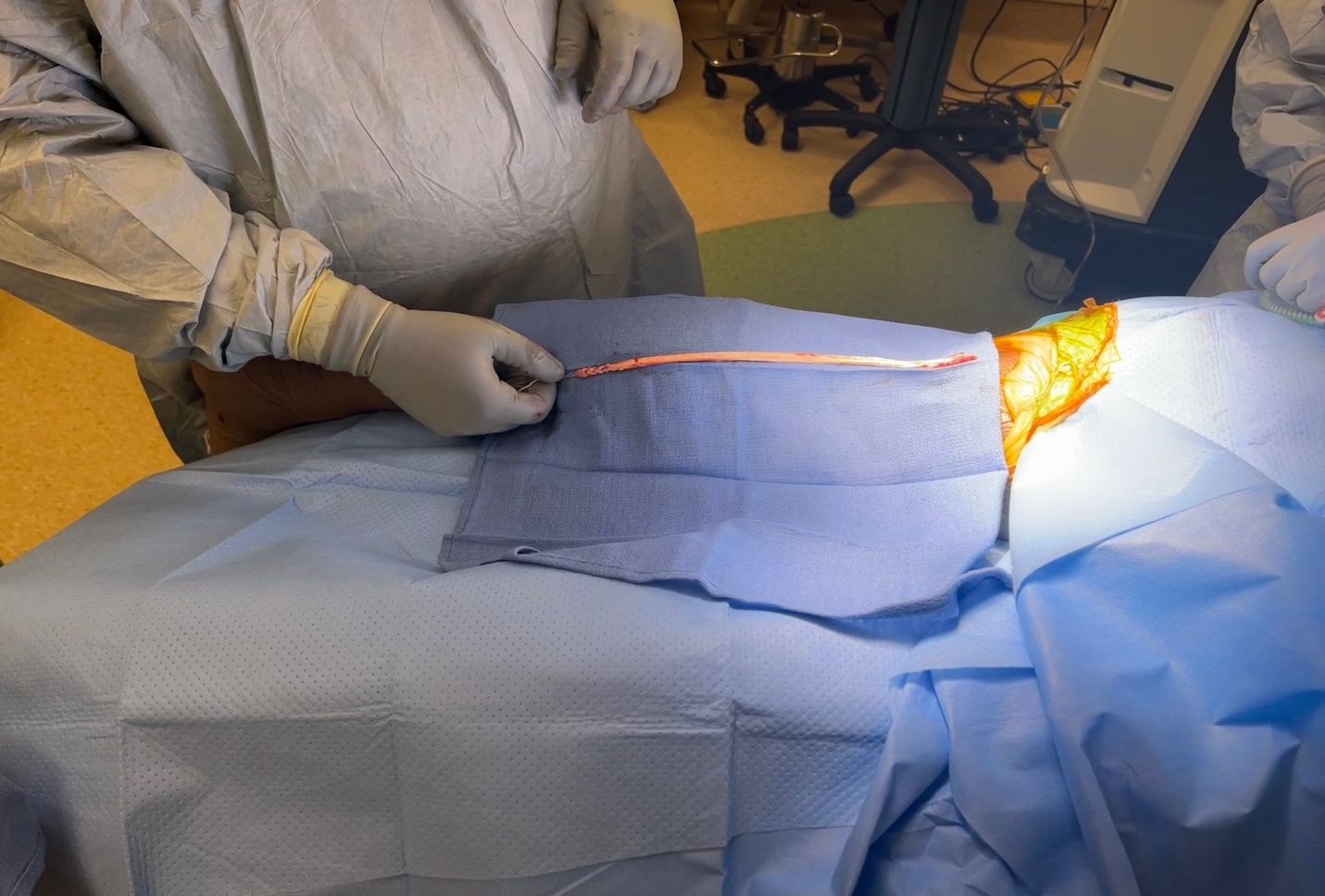
The acute hemorrhagic tendon was encountered and exteriorized. Remnants of the hypertrophied tendon were removed, and palpation was used to ensure removal proximally. A whipstitch was inserted at the distal end of the semitendinosus tendon, and a tendon stripper was used to remove the remnant of the tendon (Figure 6). The semitendinosus muscle was then placed back into the thigh at resting length. The tract was then copiously irrigated, and plasma-rich platelets (PRP) were injected into the tract to facilitate tissue healing to the semimembranosus. Subcutaneous layers were then closed with 3-0 Vicryl followed by 3-0 Monocryl and Steri-strips. A pressure dressing was applied, and the patient was then placed in a knee immobilizer.
Examination
The subject was referred to physical therapy the day after his hamstring excision procedure. The subject was weight-bearing as tolerated, ambulating with standard axillary crutches while wearing his knee immobilizer. He reported reduced daily function and posterior thigh pain during the subjective portion of his examine which were in accordance with his answers on patient reported outcome (PRO) questionnaires. During the initial examination, post-op dressings were removed to assess wound healing status and to monitor for any signs of infection. The patient noted mild tenderness to palpation around the surgical site, but the surgical incision was maintained, and no signs of observable post-op complications were observed. The patient rated his post-operative pain during the initial examination as a 4/10 on the numeric pain rating scale (NPRS), and at its worst the patient reported his pain had reached 6/10 during the past 24 hours. He described his pain as dull, achy, and local to the posterior thigh. The patient noted stiffness as a primary complaint, and this was evident in reduced range of motion upon measurement. Baseline objective measures and subjective questionnaires were taken during the initial examination and are listed in Tables 1-3. His primary goal for physical therapy was to compete in the upcoming collegiate American football season in twelve weeks.
Clinical Impression
The subject presented with normal post-operative limitations, including pain, incision-site tenderness, range of motion (ROM) limitations, functional difficulties related to strength deficits, and gait abnormalities. The subject did not exhibit any signs or symptoms in accordance with red flags that would require additional medical workup or referral. Throughout this case report, the subject attended formal physical therapy sessions twice a week, and when appropriate, completed sessions with the sports medicine staff at practice or in the weight room with his team.
Interventions
Though evidence is limited, it is generally accepted that subjects spend a brief period of time in a post-operative immobilizer, minimizing knee flexion to promote incision healing in the immediate post operative phase.9,16 While incision healing is occurring, an emphasis should be placed on mobilizing and stretching the hamstring as tolerated to prevent pathological scarring over the region.9 The structural integrity of the lower limb is not jeopardized with this procedure, thus, early, weight bearing as tolerated is recommended to aid in the rehabilitative process.16 General guidelines for rehabilitation progression combine subjective pain-ratings with various activities and exercises, and patient performance on strength and psychological readiness proxies to guide the return to sport decision-making process. A sequential progression of pain-free, or with minimal pain, walking to low-effort jogging, running to sprinting framework is generally followed while the athlete continues to build tissue tolerance and strength with exercise targeting the hamstring.37 However, given the logarithmic increase in loading of the hamstrings with sprinting velocities of 85-100%, subject tolerance to high-speed sprinting, satisfactory completion of strength and functional testing, and psychological readiness must be continuously monitored during the return to sport decision-making process.34,35
Prior to beginning physical therapy, the physical therapists (GZ, MM), athletic trainer (MR), player development staff (RH) and head team physician (KF) discussed the recommended protocol below including any precautions, time-line considerations, and criteria for progression through each phase. The protocol is available for reference in Appendix A
PHASE I – PROTECTION PHASE (WEEK 1)
The primary goals of this phase are to restore range of motion, manage pain, and to normalize motor recruitment. An emphasis on restoring any extension deficits and stretching the hamstring are recommended to prevent pathological scarring along the hamstring.9 Additionally, rehabilitation must be conducted in a manner which pain levels decrease and motor recruitment improves to ensure appropriate tissue healing is taking place. Pain avoidance with exercise is not entirely necessary, and evidence shows tissue loading below an established pain-threshold can help maintain hamstring strength and fascicle length compared to pain-free protocols.38
The first day of treatment focused on restoring knee range of motion (ROM) through heel prop and passive heel slide exercises. Additional exercises aimed at improving ROM and managing swelling included patellar mobilizations and calf pumps. Standing active knee flexion was introduced to begin normalizing motor recruitment of the hamstrings, and the subject was instructed not to exceed pain levels of >4/10 per current evidence suggesting pain levels <4/10 are acceptable in early hamstring rehab.38 Isometric quadriceps sets were introduced to begin reactivating the quadriceps muscles and to aid in maintaining full knee extension ROM. Other exercises introduced at this time included calf raises and lateral hip abduction lifts, supporting the general fitness of lower limb musculature and promoting tissue perfusion.
Additional education for the patient included techniques for managing pain and swelling, such as icing, applying compression with an Ace wrap, and elevating the leg. Post-surgical precautions were emphasized, including keeping the incision dry during bathing, sleeping with the knee immobilizer, and using both crutches and the knee immobilizer during all instances of ambulation. The patient was instructed on the proper gait sequence while using bilateral crutches and the knee immobilizer. To progress to the next phase of rehabilitation, the patient needed to achieve full, symmetrical knee extension compared to the opposite leg, attain roughly 60 degrees of knee flexion to ambulate properly, and demonstrate the ability to perform the aforementioned exercises with <4/10 pain.
PHASE II – INITIAL LOADING PHASE (WEEK 2)
The subsequent phase of rehabilitation built upon elements of the previous phase. The knee immobilizer and crutches were discharged as the incisions closed, the subject demonstrated adequate muscle activation and movement coordination with gait, and pain levels diminished with walking. Restoring full range of motion at the knee continued to be a primary focus with the goals of maintaining full, symmetrical knee extension and establishing knee flexion within 95% (120-degrees) of the contralateral side (125-degrees). Heel slides were still present in the rehab program; however, once the subject achieved 100 degrees of active assisted flexion, the recumbent bike was utilized to facilitate knee flexion and served as an entry point to aerobic energy system training.
Closed kinetic chain (CKC) movement variations using blood flow restriction (BFR) were introduced to progressively load the lower limb and to induce metabolic stress to local tissue. BFR facilitates muscular hypertrophy adaptations due to metabolite build-up caused by the hypoxic environment induced in tissues with low thresholds for mechanical stress.39 Exercises included: leg press, mini-squats, leg curl, calf raises, and lateral heel taps. The subject performed the recommended rep scheme of 30/15/15/15 with a 45-second rest between sets, with the cuff placed proximally on the subjects upper thigh and continuously inflated at 80% of occlusion. The Delfi Personalized Tourniquet System was used for BFR training in this case. The Delfi device uses sensors within an inflated pneumatic cuff to continuously measure patient blood pressure and to calibrate the limb occlusion pressure needed to restrict arterial blood flow at a percentage set by the therapist for the desired training stimulus while the patient performs exercises.40 The total time in the tourniquet did not exceed >10 minutes in any single session.41 CKC hip-hinge and hip bridge variations were also introduced to progress mechanical stress to the hamstrings, external resistance was gradually increased as tolerated while not causing the patient to exceed the recommend pain threshold of 4/10.38 To progress to the next phase the subject had to demonstrate symmetrical knee extension and flexion range of motion compared to the contralateral limb, pain-free ambulation, and <4/10 pain with previously prescribed exercises. Additionally, at this time point, the subject began strength training of the contralateral limb and upper body in the weightroom with the performance staff to minimize any deconditioning effects once the athlete discharged crutches and met the previously described Phase II exit criteria.
PHASE III – STRENGTHENING (WEEKS 3-6)
The focus of Phase III was to progress hamstring strength and tissue tolerance in movement patterns established during Phase II. Given the importance of hamstring strength in injury prevention and rehabilitation,31 a progressive periodized strength stimulus was consistently dosed in the subject’s program throughout the duration of rehabilitation. Phase III began by progressing CKC hip hinge and OKC knee flexion variations. CKC Romanian deadlifts were progressed from bilateral to unilateral to isolate the involved limb while step-ups and heel taps progressed from 8 to 20-inch boxes. External loading was appropriately added to these movements as the patient tolerated the progression. Regarding knee flexion-based movements, standing leg curls under BFR were progressed to isotonic prone leg curls against external resistance to challenge the inner range of the hamstrings, and seated leg curl variations under cable resistance were used to challenge the outer range. During this phase, a primary focus was to increase mechanical stress and elicit high levels of perceived exertion to drive adaptations of hypertrophy and strength.42,43 The criteria to advance to the next phase where the athlete would begin his running progression included: symmetrical knee flexion and extension range of motion compared to the contralateral side, <4/10 pain at the posterior knee or thigh pain with the current rehabilitation program, and a limb symmetry index (LSI) of isometric hamstring strength of >65% measured in the inner range of the hamstrings.37,38,44 By week six , the subject had achieved symmetrical knee range of motion side-to-side and rated his pain as a 0/10 with the current loading parameters of the rehabilitation program. Additionally, he demonstrated >65% LSI when measuring inner range (hip neutral with the 90-degrees of knee flexion) hamstring strength isometrically with VALD dynamometry. All performance metrics and physical examination measurements recorded at week six to initiate the athlete’s return to running phase are presented in Table 4.
PHASE IV – RETURN TO RUNNING (WEEKS 6-9)
Phase IV built on the strength capacity and tissue tolerance established in Phase III. To bridge the gap between strength training movements and high speed running, running technique drills and a walk:jog progression were introduced in the rehabilitation program during this phase.37 During this time, the subject completed running drills such as A-skips, B-skips, and various other alternating high-knee iterations to expose his hamstring to the phases of the running gait cycle. His running progression began with a walk:jog ratio of 1-minute:1-minute for 10 minutes. As the subject tolerated running technique drills and jogging intervals, the intensity and distance of running drills and jogging increased. Previous Catapult GPS data available from the subject’s participation in games and practice was used to inform his running progression. Catapult GPS allows users to track team sport athletes and record metrics including total yardage, top-end speed, and many other workload contributors.36 During this phase, the subjects running volume in yards was gradually progressed to the total yardage he normally completed during practice. However, during this phase the subject ran at submaximal intensities due to the logarithmic increase in hamstring loading with running above 80-100% speed.34,35 The criteria to progress to Phase V included: <0/10 pain at the posterior knee or thigh pain with the current moderate running volume at submaximal intensities as recommended in current evidence for high speed running.44 A limb symmetry index (LSI) of isometric hamstring strength of >85% measured in the inner range of the hamstrings and >65% in the outer range. By week nine, the subject satisfied the aforementioned criteria.
PHASE V – RETURN TO SPRINTING/SPORTS SPECIFIC DRILLS (WEEKS 9-12)
Phase V consisted of returning the athlete to sprinting, integrating into sports specific drills, and normalizing strength capacity compared to the contralateral limb and preinjury records. Additionally, an emphasis on motivational interviewing was used by the physical therapist to address any underlying biopsychosocial elements that could arise given the athlete was originally injured while sprinting. The athlete’s sprint progression was tailored to gradually progress the athlete back to his preinjury top speed velocity, top speed distance, and player load per minute as measured during previous practice sessions with Catapult GPS data. A block periodization progression was utilized during each week to gradually progress the athlete toward these metrics. During this time, the subject also began integrating into sport specific drills in practice. Drills began in a single plane without contact and progressed into multiplanar reactive contact drills as the subject continued to demonstrate tolerance to his overall workload. The final progression of this phase involved shifting the strength stimulus to focusing on eccentric muscle contractions at the hamstring. Maximizing eccentric hamstring strength has been proven to be a desirable rehabilitation outcome due to its link to performance in running-based sports.37,45 Romanian deadlift variations were progressed to overloaded single leg eccentric variations to target the hip and the use of the Nordic Hamstring Exercise (NHE) was used to primarily target hamstring capacity during eccentric knee flexion.46 The NHE has been shown to activate the hamstrings at a high level and at joint angles at which peak hamstring activation occurs during sprinting.45 For context and comparison, preinjury max values were established and taken from routine readiness and performance assessments previously conducted by the athletic training and strength staff. Eligible max metrics included values recorded within the prior six months with assessments from one month prior to the injury being the data set closest to the time of injury. criteria to return to sport after this phase included: 0/10 pain at the posterior knee or thigh pain with the current resistance exercise program, 0/10 pain or apprehension while demonstrating >95% of performance on preinjury running key metrics, hop testing on VALD Force Decks within >95% of preinjury levels on key metrics, and Nordbord eccentric max force and max impulse >65% LSI compared to the opposite side.
Outcomes
The patient reported outcome measures used and continuously tracked during this case have been presented in Table 3. The subjects FASH score improved from 43% at baseline to 90% at 12-weeks coinciding with when the subject returned to sport. An MCID value has not been established in the literature for the FASH, however, the minimum detectable change (MDC) threshold of 7.2 points was surpassed in this case. The subjects SANE improved from 10% at baseline to 85% at 12-weeks. Performance on the SANE surpassed the MCID value of 28.8% and is indicative of significant improvement in patient status by 12 weeks post-operatively. Last, the subjects OSPRO-YF scores improved with a decrease from 11 positive indicators of psychological distress to 2 at 12-weeks. Subject scores on the OSPRO-YF were indicative of a reduction in the potential presence of psychological factors related to the domains of self-efficacy and acceptance, negative pain, and negative mood by return to sport.
Repeated strength testing was completed at baseline, six, and twelve weeks post operatively. Hop testing and eccentric strength testing were initiated at week six, and, alongside GPS tracking, were monitored from baseline through return to sport. The subject’s performance improved at each time point during his rehab, and he satisfied all return to sport criteria by Week 12. All performance metrics and physical examination measurements recorded at the time of return to sport are depicted below in Tables 5- 7.
Discussion
The primary aim of this case report was to provide a framework for postoperative rehabilitation and return-to-sport decision-making following a distal semitendinosus hamstring excision in an elite athlete. Hamstring injuries are common in sports that require high-speed running, change of direction, and other explosive lower extremity movements.19 Due to high recurrence rates and variable time loss, hamstring injuries can present a significant burden to athletes returning to sport.2,3 While some athletes may opt for conservative management, a distal semitendinosus tendon excision in the presence of semitendinosus disruption or avulsion, instability, or chronic symptoms may be an adequate alternative with higher return to sport rates and less time lost.6,7,10,11 In a study by Cooper et al. 42% of elite-level athletes failed conservative treatment of distal semitendinosus rupture after an average of 16.8 weeks, requiring surgery to resect the torn tendon and surrounding scar tissue.7 In a study by Fermín et al. 92% of athletes who opted for initial surgical treatment for distal hamstring tendon injuries returned to sport while 53% of patients initially treated conservatively had to be operated on, delaying their return to sport time to a mean of 7.6 months after injury.11 Furthermore, in a study by Thompson et al., at 1-year follow up, 100% of patients were participating in their previous level of sport with 92% reporting they were “very satisfied” about the outcome of their surgery.15 To the knowledge of the authors, this is the first case report documenting a distal semitendinosus excision and rehabilitation of an collegiate American football player, and the first study to include multiple subjective, strength, and performance measures at various time points during rehabilitation.
The semitendinosus excision technique is gaining popularity as a treatment option alternative to conservative care for distal tendon pathology.9,16 In this case, PRP injection was used as an adjunct treatment due to its ability to potentially facilitate tissue healing to the semimembranosus through various pathways, shorten the time to return to sport when compared to a rehabilitation program alone, and given the easy accessibility and consistency of use in the management of hamstring pathology in elite level sports.47–49 The tendon excision procedure has yielded positive results; however, there is no current consensus on the appropriate rehabilitation protocol that should follow. Therefore, the subject followed a short period of bracing and limited knee flexion to allow for incisional healing. Early weight bearing and resistance exercise to subject tolerance was utilized to introduce loading to the knee and hamstring muscle. Closed and open kinetic chain variations of hip extension and knee flexion exercises were used with progressive loading to further prepare the tissue for the demands of running. The running program began at Week 6 and progressed to sprinting, change of direction, and agility drills by Week 9. From Weeks 9 to 12, the athlete continued to work with the rehabilitation team and coaching staff while integrating back into full practice until he passed all of his return to sport criteria. Once he passed all his return to sport criteria, he was able to participate in football-related activities and competition at 12 weeks post operatively.
The physical readiness measures in this case included strength, hop, and GPS metrics, all of which were objectively determined. When cleared, the athlete’s performance on the Nordbord eccentric leg curl test indicated an LSI of 66.1% and a 34.8% strength deficit compared to the athlete’s pre-injury max (Table 5). Due to the remaining deficits, the subject did not participate on the special team unit after clearance was granted in attempt to limit exposure to straight line top speed sprinting in game conditions. Six weeks after returning to competition, the athlete demonstrated a max force LSI of 85% when compared to the contralateral side and a strength deficit of 11% when compared to the pre-injury max value. The subjects in-season increase in hamstring strength was encouraging; however, it is difficult to determine if the tendon excision procedure will result in long-standing knee flexion weakness at this time like that of what is observed in populations with similar pathology.
The FASH, SANE, and OSPRO-YF questionnaires improved at each time point except for the FASH between baseline (43%) and six weeks (32%). The authors of this manuscript speculate this perceived decline in function may have occurred due to the time point coinciding with the subjects first exposure to the Nordbord eccentric curl exercise post injury. The subjects initial Nordbord performance was significantly less than his previously established max, this could potentially have fostered a perceived decline in function from the athlete.
There are several limitations for this case report. First, it includes only one participant, which is typical for case reports. Additionally, the follow up after returning the subject to sport was brief, lasting only a few months due to the athlete participating in the collegiate American football season, thus, long-term outcomes are unknown at this point. Due to the constraints of the collegiate season a prolonged reconditioning and testing battery of the athlete’s eccentric hamstring strength was unable to be deployed. The presence of hamstring strength deficits after an athlete has returned to sport following a strain or tear is well documented in the literature, similar deficits are also observed after ACL reconstructions where the patient utilizes a hamstring autograft.31,32,50 Given the presences of these deficits there is a possibility that compensation strategies influenced the results of the athletes return-to-sport testing. This may limit the validity of the return to sport battery in determining the true readiness to return to sport. Last, the findings from this case report are not applicable to other patient populations with distal semitendinosus tendon excisions as the case report design does not establish a cause-and-effect relationship. Nevertheless, this case report is valuable in illustrating the clinical decision-making process and outlining the rehabilitation progression for an elite-level male American football player who underwent a distal semitendinosus tendon excision.
Conclusion
The results of this case report highlight the successful return to sport of an elite-level collegiate American football player twelve weeks after a distal semitendinosus tendon excision and structured rehabilitation. The findings are intended to inform physical therapists, athletic trainers and orthopedic surgeons and provide a proposed protocol to guide the rehabilitation for patients following a semitendinosus excision. Future research should focus on larger-scale studies to further examine the effectiveness of the suggested guidelines in elite-level athletes.
Corresponding Author:
Giorgio Zeppieri Jr.
Department of Rehabilitation, University of Florida
University of Florida, Gainesville, FL 32608
Email: zeppig@shands.ufl.edu
Subject Consent
The subject was informed prior to treatment that data concerning the subject would be submitted for publication.
Resident Case Report
Case report was completed during the University of Florida Health Sports Residency approved by the American Board of Physical Therapy Specialties (ABPTS).
COI
The authors have no conflict of interest to disclose.