INTRODUCTION
Over the past 20 years, Anterior Cruciate Ligament (ACL) injuries have risen significantly among school-aged children and adolescents, with an estimated 121 injuries per 100,000 annually.1 Injury rates peak in both girls and boys during high school, with girls reaching a rate of 392 per 100,000 person-years at age 16 and boys a rate of 422 per 100,000 at age 17.1 In children and adolescents, surgical treatment has been shown to be more favorable with less likelihood of a future meniscal tear or instability and improved ability to return to prior level of play when compared with conservative management.2
Following Anterior Cruciate Ligament Reconstruction (ACLR) as few as 73% of adolescents are able to return to their primary preinjury sport within two years following ACLR.3 More troubling is that for those who do return, nearly one third will sustain a second ACL injury.4 Though successful outcomes following ACLR are multifactorial, restoring the strength of the knee extensors is a key component of post-operative rehabilitation. In the short-term, symmetrical knee extensor strength has been linked to patients’ ability to return to sports and to reduced secondary injury risk.5–7 In the long term, more symmetrical strength of the knee extensors is associated with improved overall knee health and physical activity.8,9 Unfortunately, the restoration of knee extensor strength remains one of the more challenging aspects of ACL rehabilitation.10 For this reason, finding which interventions can most effectively restore post-operative strength of the knee extensors is critical.
Blood flow restriction training (BFRT) is an adjunct to strength training that has grown in popularity amongst physical therapists (PTs) used to facilitate strength recovery after ACLR. BFRT uses a cuff or tourniquet on a limb to reduce arterial inflow and occlude venous return. Thus, creating a hypoxic environment with exercise that has been theorized to promote muscle hypertrophy through altered cell signaling, increased protein synthesis, and stem cell proliferation.11 Several studies have shown that performing low load resistance training with BFRT can increase muscle strength and hypertrophy following ACLR in adults.12–14 There is also preliminary evidence suggesting that BFRT may be beneficial in the adolescent population, as BFRT groups showed higher isometric knee extension peak torque at both three months post operatively and during return to sport testing on both the ACLR and uninjured limbs than control groups.15
While research evaluating the effectiveness of BFRT is growing, the specifics regarding application of BFRT within clinical settings remains unknown. Understanding how BFRT is used and what exercise prescription is followed in the pediatric and adolescent population is necessary to understand if there is concordance between research and clinical practice. Therefore, the purpose of this study was to describe the influence of patient clinical presentation on BFRT use and exercise prescription in pediatric and adolescent patients after ACLR.
METHODS
Survey Development
A team of three PTs (N.G.G, E.M.G, L.S.B) collaborated to develop an electronic survey using REDCap electronic data capture tools.16,17 Each of the developers had greater than 15 years of physical therapy experience with adolescents following ACLR and were BFRT certified (N.G.G. and E.M.G. through Owen’s Recovery Science and L.S.B. with Smart Tools). Development of the survey started with identifying key patient presentations specific to ACLR rehabilitation that may impact decision making regarding the prescription of BFRT. Following initial survey development, the survey was pilot tested with three additional PTs representative of the target sample. Feedback was collected and modifications were made to improve clarity and reduce completion time.
The final survey consisted of three sections: (1) clinician demographics and clinical practice settings, (2) BFRT training or educational coursework, and (3) clinical decisions related to BFRT prescription in response to patient-specific factors such as age, pain, time from surgery, weight bearing status, effusion and range of motion (ROM). To understand clinical decisions, participants were presented with a series of case vignettes that varied in patient factors that may affect BFRT prescription. Case vignettes are detailed in Table 1, with the full survey available in the Appendix. The survey took approximately 10 minutes to complete.
Participants
A convenience sample of PTs who rehabilitate pediatric and adolescent patients after ACLR were recruited for participation via email and social media. Rehabilitation continuing education providers sent out an email with the link to the REDCap survey and study flyers were posted on social media. Participants were encouraged to share the study flyer with their peers, facilitating snowball sampling. All responses were anonymous and no identifiable information was collected during the survey. This study received approval from the primary authors institutional review board.
Statistical analysis
Descriptive statistics were utilized to summarize frequency of responses. Data were analyzed by comparing frequency distribution among survey responses using Microsoft Excel 2016.
RESULTS
Participant Demographics and Experience
The survey was opened by 215 participants, with 147 PTs completing the entire survey. There was a diverse representation of geographic regions, practice settings and years of PT experience among the participants. Participants’ demographic and experience profiles are shown in Table 2.
Age-Related Decision Making
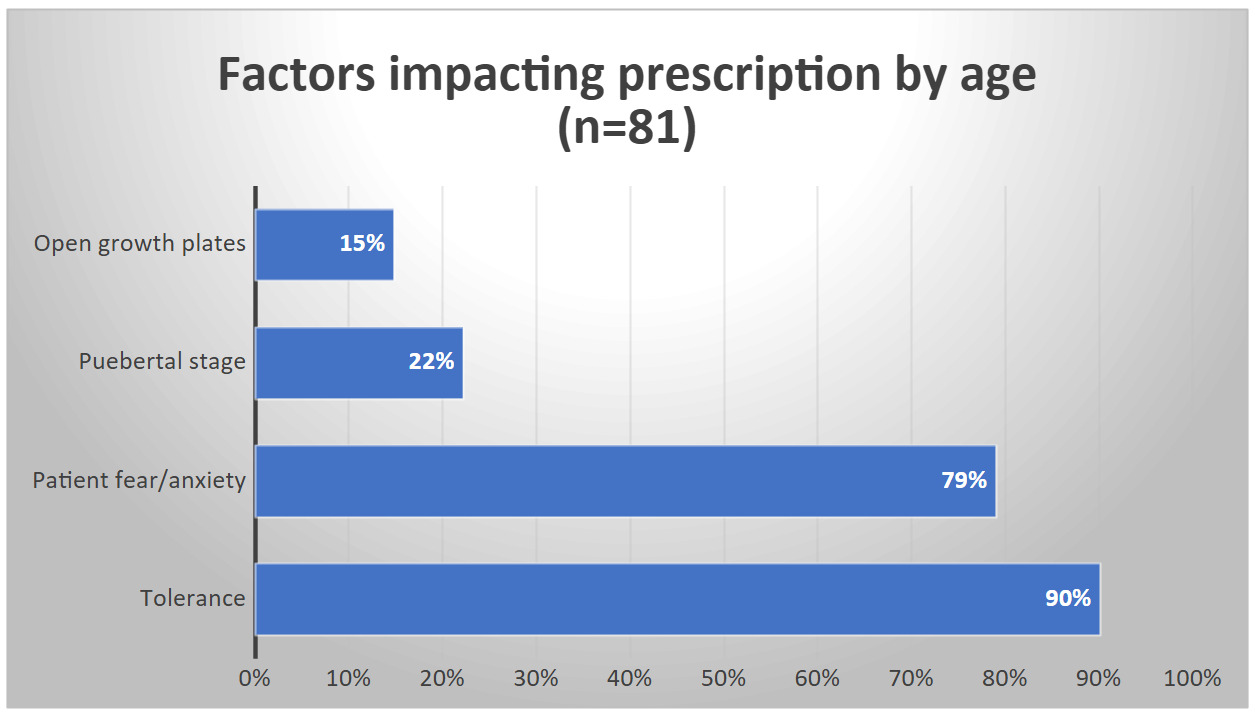
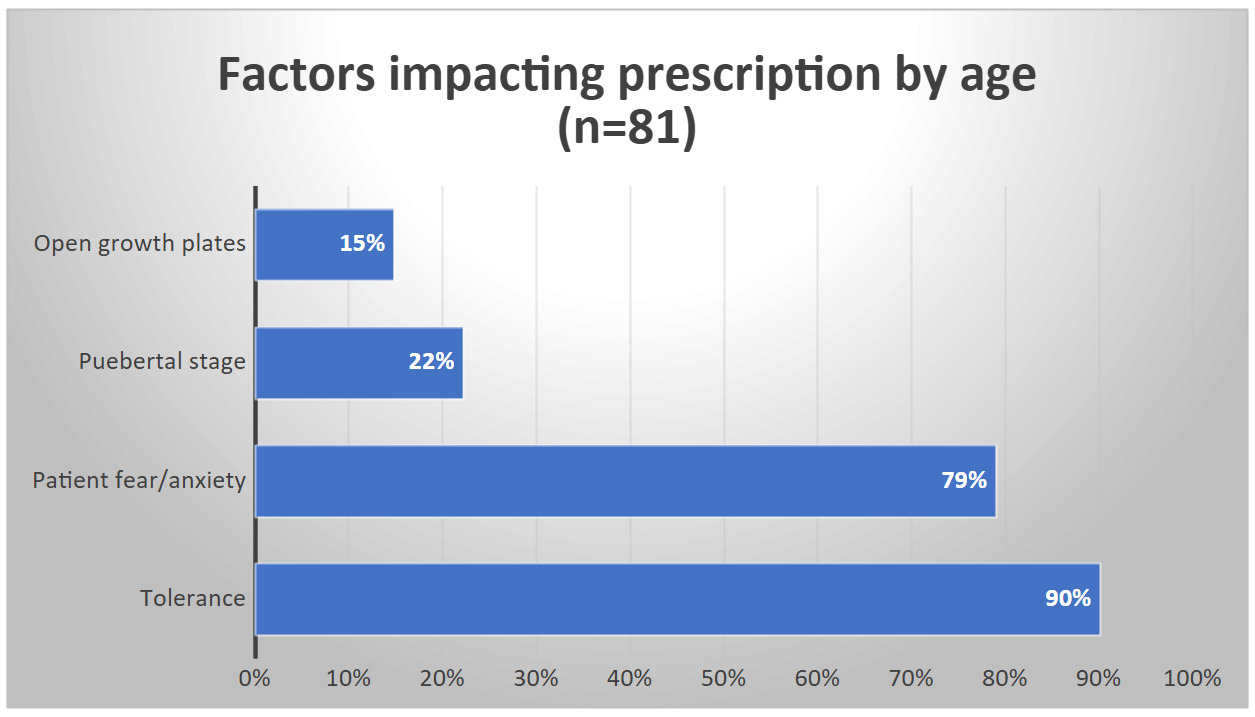
A total of 55% of participants indicated that they would not use BFRT on younger patients. Among those, 90% cited concerns related to patient tolerance, 79% reported concerns of patient fear or anxiety, 22% noted concerns with pubertal stage or hormonal factors, and 15% expressed concern about potential damage to open growth plates (Figure 1).
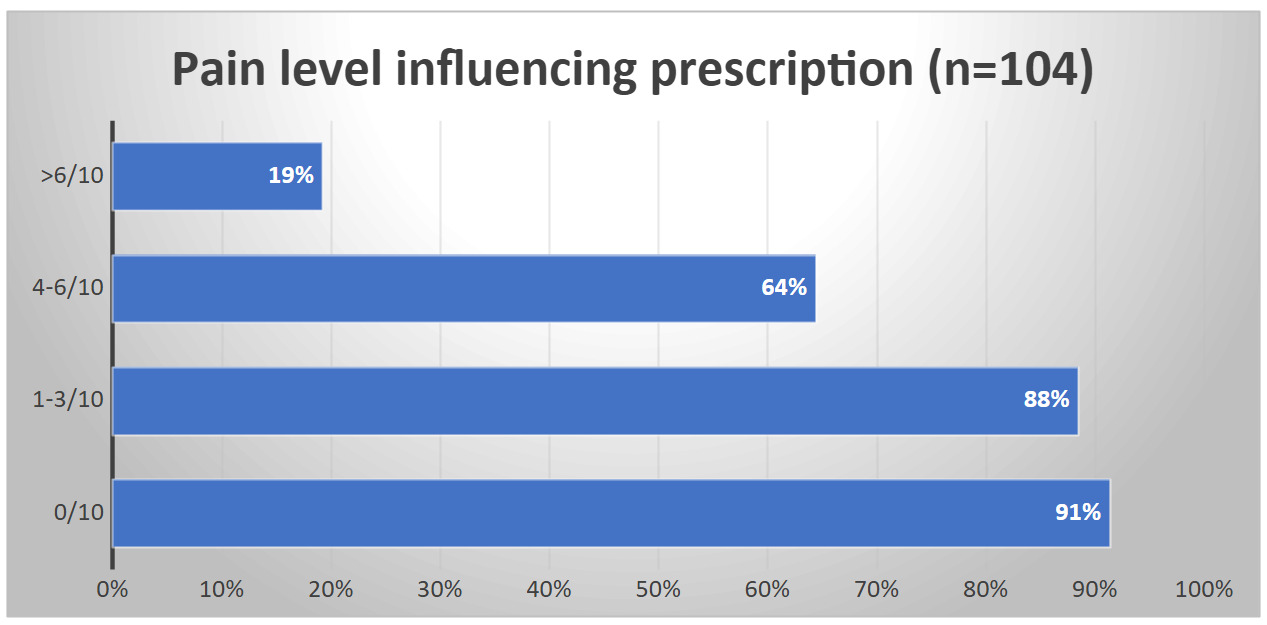
Pain-Related Decision Making
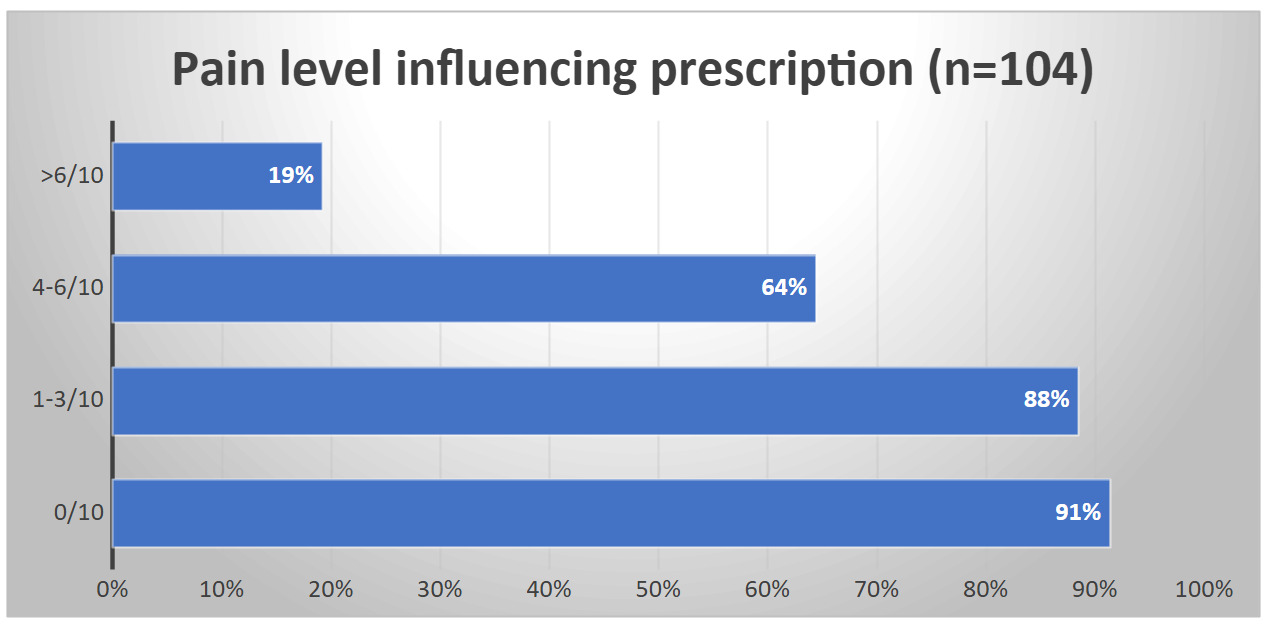
When asked if pain impacted choice regarding BFRT application, 71% of participants responded yes. While, 91% indicated that they would use BFRT when there was no pain, increasing pain levels on the numeric pain rating scale resulted in decreased frequency of BFRT use. A total of 88% would use BFRT with pain ranges of 1-3/10, 64% with a pain range of 4-6/10, and 19% when pain level was greater than 6/10 (Figure 2).
Preoperative Use of BFRT
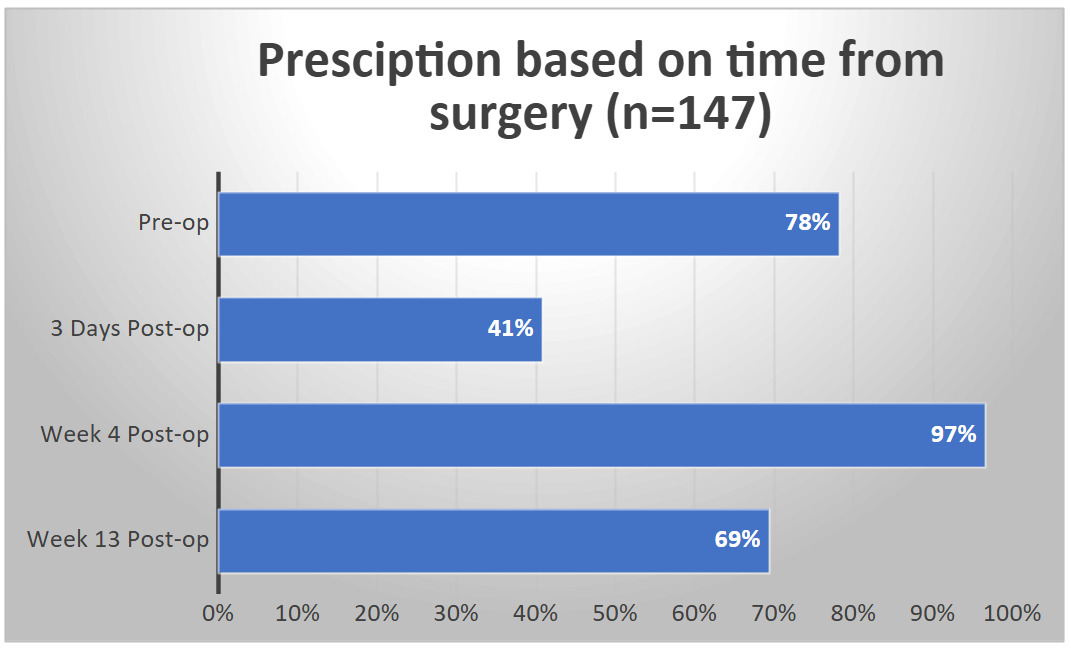
Preoperative BFRT utilization was reported by 78% of participants (Figure 3). Patient characteristics related to knee effusion were most influential in BFRT utilization pre-operatively, with 63% of respondents indicating the presence of a knee effusion would move them to not utilize BFRT. ROM limitations were less influential, as 77% of participants who prescribed BFRT preoperatively would continue to use it despite ROM limitations of flexion to 70 degrees and extension lacking 15 degrees.
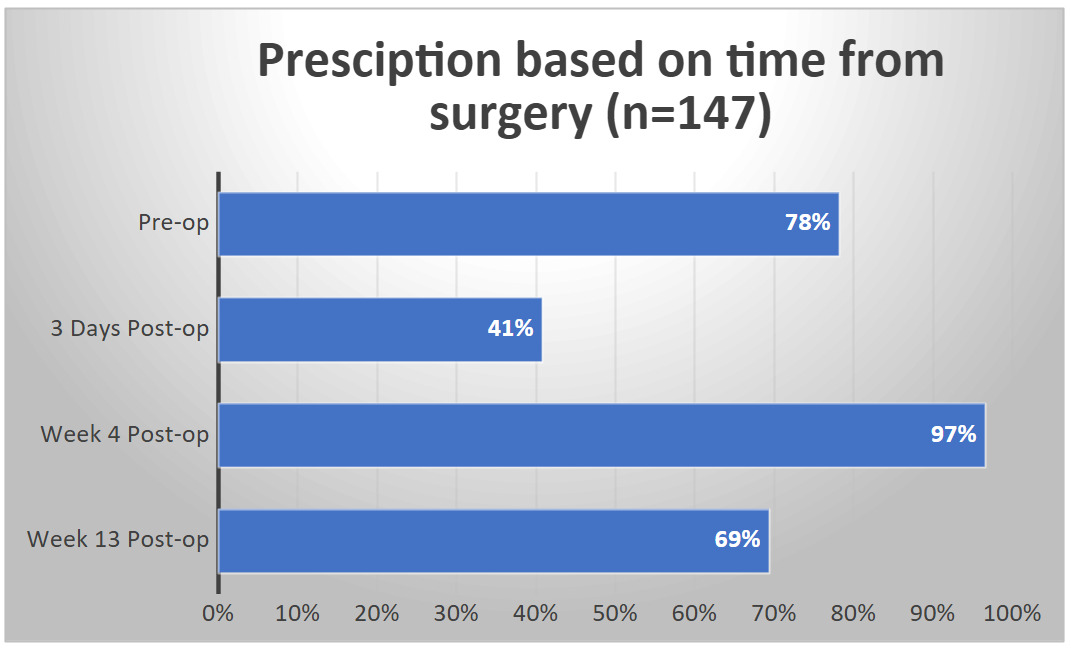
Postoperative Use of BFRT
Postoperative prescription patterns varied across time points. Participants were most likely to use BFRT at week 4 postoperatively (97%), followed by week 13 (69%), and least likely on postoperative day 3 (41%) (Figure 3). BFRT utilization was affected by level of knee effusion during the early recovery period after surgery. At postoperative day 3, 53% of participants who reported using BFRT at this time point, would discontinue use of BFRT if the patient had a knee effusion of 2+ or more. Similar to preoperative trends, 88% of those prescribing BFRT at postoperative day 3 and week 4 reported they would continue use despite ROM limitations. BFRT use was generally consistent regardless of weightbearing status; only 3% of participants reported that they would modify BFRT use if a patient were non-weightbearing compared to weightbearing as tolerated.
Discontinuation of BFRT
Only 52% of participants indicated that they have defined criteria for discontinuing BFRT. Among those, quadriceps strength limb symmetry index (LSI) thresholds commonly guided discontinuation with 18% discontinuing at >70% LSI, 37% at >80%, and 33% at >90% LSI. Smaller proportions reported thresholds of >60%, >50%, or 100% LSI (each 4%). Additionally, 54% of respondents stated they would discontinue BFRT once the patient demonstrated good movement quality conducive to external loading.
DISCUSSION
The results of this study revealed that patient age, joint effusion and time from surgery were important considerations that impacted PTs decisions on use and prescription of BFRT in pediatric and adolescent patients. Interestingly, changes in knee ROM and weight bearing status did not affect BFRT prescription patterns. While other studies have surveyed practitioners about their use of BFRT, to the authors knowledge, this is the first to examine clinical decision making as it relates to the intervention.18–21
Regarding age, concerns related to patient tolerance, fear, and anxiety were the clinical factors that deterred the majority of PTs from prescribing BFRT. Though evidence of patient tolerance is limited in the adolescent population, a small cohort of adolescent patients following ACLR showed good tolerance to BFRT.22 In this study 29 subjects underwent 535 BFRT sessions with only 56 (10.47%) occurrences of being unable to finish the treatment session and only 19 (3.55%) needing to decrease limb occlusion pressure. Furthermore, the authors identified a limitation in how inability to finish was defined, which included voluntary stoppage of exercise by the patient or the inability to complete all 75 repetitions in eight minutes. Which may have caused an overestimation of patient intolerance. While it was a small study, it does offer preliminary evidence that BFRT may be well tolerated among this population.
PT concerns related to physiological development and hormones also appeared to influence decision making. While the results of the current study are unable to elucidate why PTs altered their BFRT prescription decisions, the authors hypothesize these decisions may be based on several factors. One factor may be the known differences in how strength is attained from childhood to adulthood. Prior to puberty, low levels of testosterone, growth hormone, and insulin-like growth factor limit the ability to increase muscle size.23 At this point in development, increases in strength come primarily from an increase in the number of motor units activated.24 In a healthy adult population, BFRT has been shown to increase the activity of motor units with higher action potential amplitudes, which could offer benefits to youth patients using this intervention.25 However, there are no studies exploring this mechanism of action within children or adolescents. PTs also demonstrated disagreement on BFRT prescription with consideration to the presence of open growth plates. Open growth plates are precautions for modalities such as ultrasound and electrical stimulation, but at this time there is no consensus as to whether open growth plates should serve as a precaution or contraindication to BFRT.26 Metabolic, hormonal, and hematologic abnormalities can cause growth arrest and are a valid concern for the long-term safety of BFRT use. Research has indicated that use of BFRT may be associated with alterations of concentration of testosterone, growth factor and insulin-like growth factor in adult male populations.27 Once again, this effect of BFRT has not been directly studied in children or adolescents and may represent a valid concern for side-effects within developing athletes. However, it should be noted that the hormonal changes with BFRT have been shown to be similar to those in high load resistance training which the National Strength and Conditioning Association recommends for school aged children.28,29 Together, these findings illustrate a need for future studies focused on younger populations to fully understand the effects of these factors and to establish a complete safety profile for BFRT in this population.
The perception of pain was another clinical factor that impacted BFRT prescription for a high percentage of participants. Participants reported that they would use BFRT with patients who reported minimal or no pain more frequently than they would for patients with higher levels of pain. This finding contrasts with the literature which shows reductions in knee pain during BFRT use and 24 hours after the intervention in patients following ACLR.30,31 With 70% of participants having formal BFRT training, it is surprising that this disconnect exists. This may highlight an important area for BFRT education improvement targeting effectiveness of this intervention for pain reduction. However, this finding may also highlight the issues of knowledge translation with practitioners not aware of most recent evidence surrounding BFRT use in pain management.
Many researchers have attempted to identify the optimal time frame for initiating BFRT after ACLR, however no consensus currently exists.32 The lack of specific guidelines seems to be reflected in this study’s results showing significant variability in how PTs use BFRT when time from surgery was manipulated. The majority of PTs indicated they would use BFRT beginning at post-op week 4. While the authors cannot ascertain motivating factors for prescription in the current study, it is hypothesized that the decision to initiate BFRT at this time point, may be related to PTs tendency to adjust use of BFRT based on patient pain levels. Around post-op week 4 most of the acute effects of post-surgical pain have resolved, which may make PTs more likely to initiate BFRT at this time. It is interesting that approximately half of participants would use BFRT beginning on post-operative day 3. Although practical barriers, such as difficulty scheduling patients early after surgery may limit BFRT prescription this early in recovery, some studies have shown a beneficial effect.13,33 Future studies exploring optimal timing for post-operative initiation of BFRT within the adolescent population are needed to guide clinicians and optimize clinical practice.
The presence of knee joint effusion had a relatively strong impact on BFRT decision-making with a range of 27-53% of participants opting to not utilize BFRT when the patient case was manipulated to present with knee effusion at various post-operative time points. While there is literature demonstrating in adults that eight weeks of BFRT may reduce knee effusion compared to high-load training, the clinicians’ decision to utilize BFRT in the presence of effusion may be based on several other factors and may reflect a preference to direct treatment for effusion more towards traditional modalities like electrical stimulation and cryotherapy.12,34–36 Interestingly, knee ROM limitations had a limited influence on BFRT utilization, with fewer than one quarter of participants adjusting BFRT prescription due to post-operative ROM deficits. Although the effects of BFRT on ROM post-ACLR are not well studied, evidence from meniscectomy patients suggests BFRT may improve ROM, indicating a need for further research in the ACLR population.37
Finally, there was considerable variation noted for criteria to discontinue the use of BFRT, with approximately half of the sample reporting using no criteria to make this determination. The most widely cited use for BFRT within rehabilitation is the ability to provide a strengthening stimulus when a patient is unable to safely engage in strength training with adequate loads (>70% 1 rep max). Experts recommend that practitioners should defer to high load strength training once the patient is able to safely tolerate this level of training.38 However, specific guidance on what patient characteristics indicate readiness for cessation of BFRT is lacking in the literature, which may explain why clinicians within the current study showed large variation and limited agreement in practical consideration of stopping the use of BFRT. Future research should seek to identify optimal duration for BFRT use and establish clinically accessible criteria to guide decision making for discontinuing this intervention after ACLR.
Limitations
This study is not without limitations. The survey used did not have a reliability analysis or content validity established, thus it is unknown if participants answered the questions as intended, potentially impacting the internal validity of the study. Because the purpose of this study was to describe the influence of patient clinical presentation on BFRT use, the authors did not account for the type of BFRT system, cuff style, width or length. These factors may have played a role in the PTs decision use BFRT as these factors shown to achieve venous occlusion with the lowest possible pressure which is considered to be safest for BFRT.39 Similarly, the cases did not indicate if there were specific monitoring protocols for physeal stress which may have impacted the results of this study. The authors used a sampling methodology of emailing via continuing education resources and snowballing social media posts may have introduced bias. As a result, around two-thirds of participants reported completing BFRT continuing education coursework, with close to two-thirds completing coursework by the same provider. Similarities in BFRT training among participants may have reduced the variability in responses and impacted the generalizability of findings. Lastly, the authors were unable to determine the clinical reasoning behind the decisions made by the participants due to this type of survey, limiting detailed understanding of the responses.
CONCLUSION
This study provides insight into clinical decision making regarding the use of BFRT in adolescent patients after ACLR. Overall, the results of this study indicate that younger age, increased reported pain, greater joint effusion, and time from surgery influenced decision making. However, ROM and weight bearing status did not appear to impact BFRT prescription. Additionally, no consistent criteria were reported regarding decision making to discontinue the use of BFRT. These findings support the need for additional research to identify optimal BFRT application within common clinical scenarios, which will help standardize practice and support clinical decision making when utilizing BFRT in adolescents after ACL reconstruction.