Concept #1: Knee Loading Varies Between Weight Bearing Exercise (WBE) and Non-Weight Bearing Exercise (NWBE)
Cruciate Ligament Rehabilitation
Regarding ACL loading between WBE and NWBE, peak ACL strain and tensile loading is greater in NWBE seated knee extension than most WBE.1–11 For example, performing stair climbing, forward lunging, and a leg press type exercise with 40% bodyweight resistance all produced less ACL strain compared with performing a seated knee extension with no external resistance.4,9,10 Interestingly, performing a NWBE seated knee extension with no external resistance, produced the same amount of ACL strain compared with performing a one leg sit-to-stand or stair climbing WBE, with WBE being more effective in recruiting important hip and thigh musculature that help stabilize the knee and protect the ACL.4,10 For NWBE, peak ACL loads have been reported to be 158 N at 15º knee angle for the 12-RM isotonic seat knee extension and 254-396 N at 35-40º knee angles for the isometric and isokinetic seated knee extension.4,11 These are higher than peak ACL loads during WBE, including 0-28 N at 25º knee angle for the bodyweight squat and 12-RM barbell squat, 0 N for the 12-RM leg press, 59-142 N at 30º knee angle for the bodyweight and 12 repetition maximum (12-RM) dumbbell one-leg squat, and 253 N at 33-48º for a two-feet drop landing stepping off a 60 cm high platform.1–8,11–13 As a reference, peak ACL load during level walking is 303 N at 15-20º knee angles.14 Therefore, WBE minimizes ACL strain or tensile loading to a greater extent compared with the seated knee extension NWBE. Moreover, WBE are more functional multi-joint, multi-muscle exercises effective in developing important hip and thigh musculature, such as the gluteals, hamstrings, quadriceps, adductors and abductors, whereas the seated knee extension only targets the quadriceps.
Since most ACL injuries are not isolated injuries and often involve bone bruises and cartilage damage, menisci damage, or collateral ligament injury, tibiofemoral compressive loads also need to be considered when selected lower extremity exercises after an ACL injury, repair, or reconstruction. For example, performing 12-RM squatting and lunging exercises, or performing a two-leg drop jump from a 60 cm platform height, all resulted in tibiofemoral compressive loads between 4-8 times body weight, which could be injurious to the healing bone, cartilage, or meniscus.1–3,6–8,13 Performing squatting or lunging type exercises with bodyweight only should be first performed and then progress to external resistance secondary to less tibiofemoral compressive knee loading occurring using bodyweight only as resistance compared to using an external load.15,16 Therefore, lower-intensity resistance and plyometric exercises should precede higher intensity resistance or plyometric exercises, such as the single-leg drop jump or 12-RM squatting and lunging. The rate of deceleration should also be considered when performing plyometric exercises, as a higher deceleration rate results in greater ACL loading. A peak ACL load of 1294 N at 25-30º knee angles has been reported during rapid deceleration during running to a stop.17
Regarding PCL loading between WBE and NWBE, peak PCL tensile forces were greater in the seated knee flexion isometric and isokinetic NWBE (2701-3330 N at 90º knee ankle) compared to WBE, including 12-RM barbell squat (1868-2212 N at 63-77º knee angles), 12-RM leg press (1726-1866 N at 88-95º knee angles), 12-RM one leg dumbbell squat (414 N at 90º knee angle), 12-RM wall squat (757-786 N at 80-90º knee angle), 12-RM forward and side lunge (612-765 N at 60-90º knee angles), and the bodyweight forward and side lunge (317-334 N at 60-80º knee angles).2,4–8,11 PCL loading during the knee extension NWBE is less than the knee flexion NWBE but greater than most WBE, with the 12-RM isotonic seated knee extension producing a peak PCL force of 959 N at 79º knee angle,2,4,5 which was greater than all the aforementioned WBE except the 12-RM barbell squat and 12-RM leg press. As a reference, the peak PCL load during level walking is 160 N at 15-20º knee angles.14 As a general rule, NWBE and WBE should first begin with no external resistance (resulting in less ACL and PCL loading) and progress to increasing amounts of external resistance (resulting in more ACL and PCL loading).
Patellofemoral Rehabilitation
When comparing WBE (12-RM squat and 12-RM leg press) to NWBE (12-RM seated knee extension), patellofemoral force and stress was greater in WBE than NWBE for 85-95º knee angles, but greater in NWBE than WBE for 15-57º knee angles.2
Concept #2: Knee Loading Varies With Technique Variations Within WBE or NWBE
Cruciate Ligament Rehabilitation
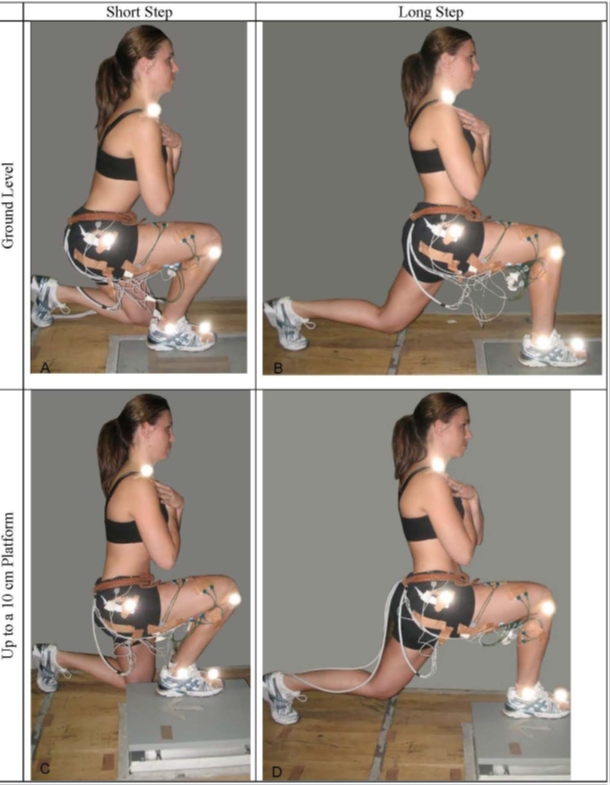
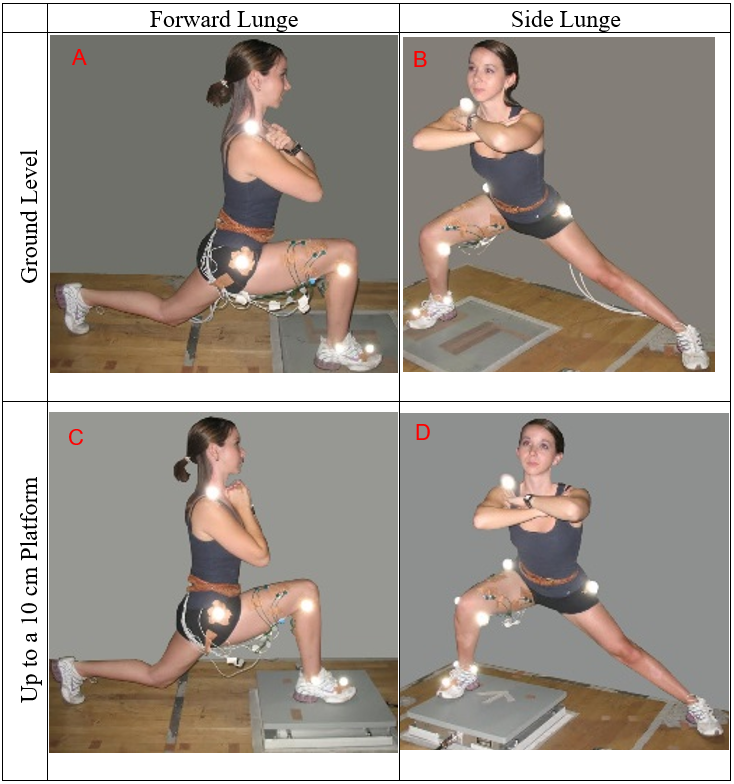
Forward and side lunge exercises can be performed with varying technique variations using bodyweight only or external resistance, such as a 12-repetition maximum (12-RM) load, and the amount of resistance used does affect cruciate ligament loading. As shown in Figures 1A-1D, the forward lunge can be performed on either a flat surface (Figures 1A and 1B) or up to a platform (Figures 1C and 1D), and by taking a long step (results in lead knee being over lead ankle at maximum knee flexion), which is referred to as forward lunge long (Figures 1B and 1D), or by taking a short step (results in knees moving forward over toes approximately 8-10 cm), which is referred to as forward lunge short (Figures 1A and 1C).
_a_short_step_at_ground_level__(b)_a_long_step_at_ground_level__(c)_.png)
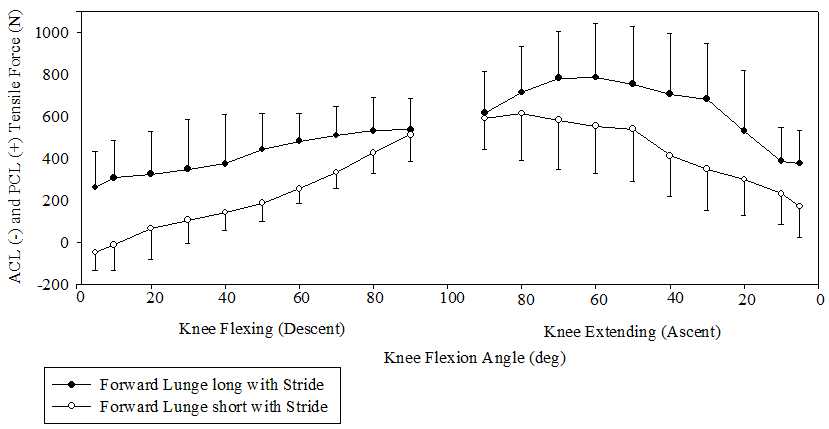
Using a 12-RM load, mean PCL forces were significantly greater (p < 0.001) between 0-80° knee flexion angles in the forward lunge long with a stride (step forward and push back to starting position) compared to the forward lunge short with a stride (Figure 2).7 Moreover, between 0-20° knee flexion angles mean PCL forces were significantly greater (p < 0.001) without a stride (lunging up and down with feet stationary) compared to with a stride.7 Mean ACL forces were generated (0-50 N range between 0-10° knee flexion angles) only in the forward lunge short with a stride (Figure 2).7
_acl_and_pcl_tensile_force_between_forward_lunge_long_and_short_with_a_stride_(st.png)
Peak ACL strain was not significantly different between squatting with or without 136 N of external resistance, or between stair climbing at slower versus faster rates.10,18,19 It can be concluded from these WBE data that increasing resistance during the squat, or increasing the rate of stepping during stair climbing, may not increase ACL strain; however, the technique employed during the squat will influence ACL loading. This may occur because adding resistance or stepping faster may affect muscle recruitment patterns, such as recruiting the hamstrings to a greater extent (perhaps owing to changes in technique, such as a greater forward trunk tilt). Muscle force from the hamstrings helps unload the ACL owing to their posterior directed force on the leg. This finding during WBE (eg, squatting and lunging), is different compared with the seated knee extension NWBE, in which ACL strain increased from 2.8% without external resistance to 3.8% with adding only 45 N (10 lbs) of external resistance.9 One possible explanation for this is that technique variations typically do not occur during the seated knee extension exercise (and the hamstrings are not recruited to unload the ACL), but techniques variations do occur during WBE, such as with the squat and lunge, because trunk position may change, such as the trunk being more vertical (more quads, less hamstrings) or more horizontal (more hamstrings, less quadriceps).
If technique variations do occur during the seated knee extension NWBE, ACL tensile force can also be affected. For example, when a constant external torque is being applied at the knee, ACL force decreases when the resistance pad is moved more proximal up the leg towards the knee compared to when the resistance pad is moved more distal down the leg towards the ankle.20 When a constant external torque was applied at the knee at 30º knee angle, the ACL tensile force was approximately twice as great when the resistance pad was positioned near the ankle (approximately 400 N) compared with when the resistance pad was positioned near the middle of the leg (approximately 200 N).20 Also, ACL loading decreased progressively from 15º knee angle (approximately 500 N when the resistance pad was near the ankle and approximately 325 N when the resistance pad was placed near the middle of the leg) to 60º knee angle (approximately 100 N when the resistance pad was near the ankle and approximately 0 N when the resistance pad was positioned near the middle of the leg), with no ACL loading at knee angles greater than 60º.20 Wilk and Andrews21 have reported that in ACL-deficient knees during isokinetic exercises, anterior tibial translation can be reduced by utilizing a proximal resistance pad position and performing higher knee angular velocities (e.g. 180 º/s and 300º/s) compared to using slower knee angular velocities (e.g. 60 º/s).
Performing the forward and side lunge by stepping forward or sideways and then pushing back to the upright starting position produced significantly greater PCL tensile force compared to performing the forward and side lunge while keeping both feet stationary and simply lunging up and down by flexing and extending the lead knee.8 Therefore, there are different progressions within the forward and side lunge that can be employed during PCL rehabilitation.
Technique variations during the leg press can also affect PCL loading. During the 12-RM leg press, mean PCL force was 11-13% greater in the wide stance leg press than the narrow stance leg press between 33-85º knee angles.2 No significant differences in PCL loading were found between the narrow and wide stance squat.2
Patellofemoral Rehabilitation
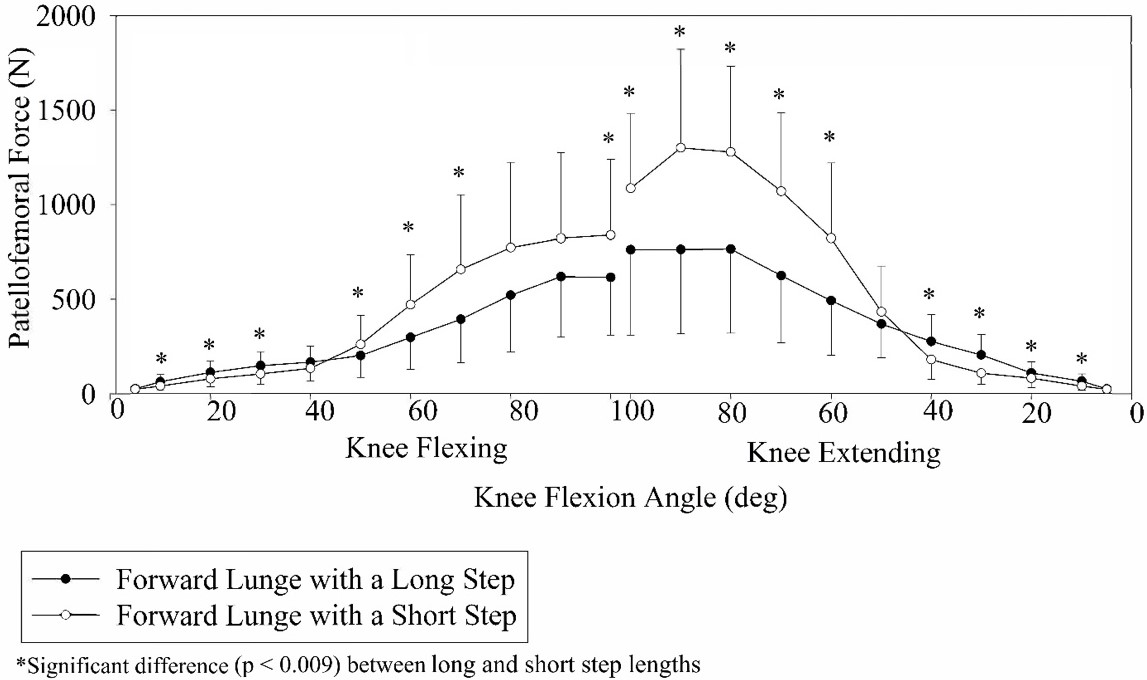
Technique variations within WBE has also been shown to affect patellofemoral loading. While performing the bodyweight forward lunge exercise with step length and step height variations (Figures 1A-1D), patellofemoral joint loading changed according to step length, step height, and knee angle.16 Specifically, patellofemoral force and stress in the lead knee were greater with a long step forward lunge (forward lunge long) compared to a short step forward lunge (forward lunge short) between 10°–40° knee angles, and greater with the forward lunge short than the forward lunge long between 50°–100° knee angles (Figure 3).16
_patellofemoral_compressive_force_in_lead_knee_for_forward_lunge_with_a_long_step.jpeg)
For the 12-RM forward lunge, patellofemoral force and stress in the lead knee were greater with the forward lunge short than the forward lunge long between 70°–90° knee angles (Figure 4).22 Interestingly, performing forward lunge with bodyweight only (Figure 3) compared to with a 12-RM load (Figure 4) did change the overall pattern of patellofemoral loading as a function of knee angles.
_patellofemoral_joint_compressive_force_in_lead_knee_for_the_forward_lunge_long_.png)
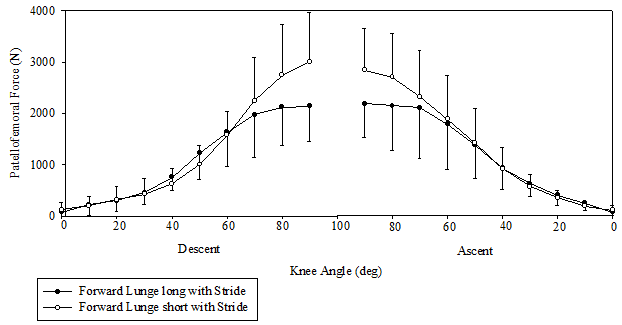
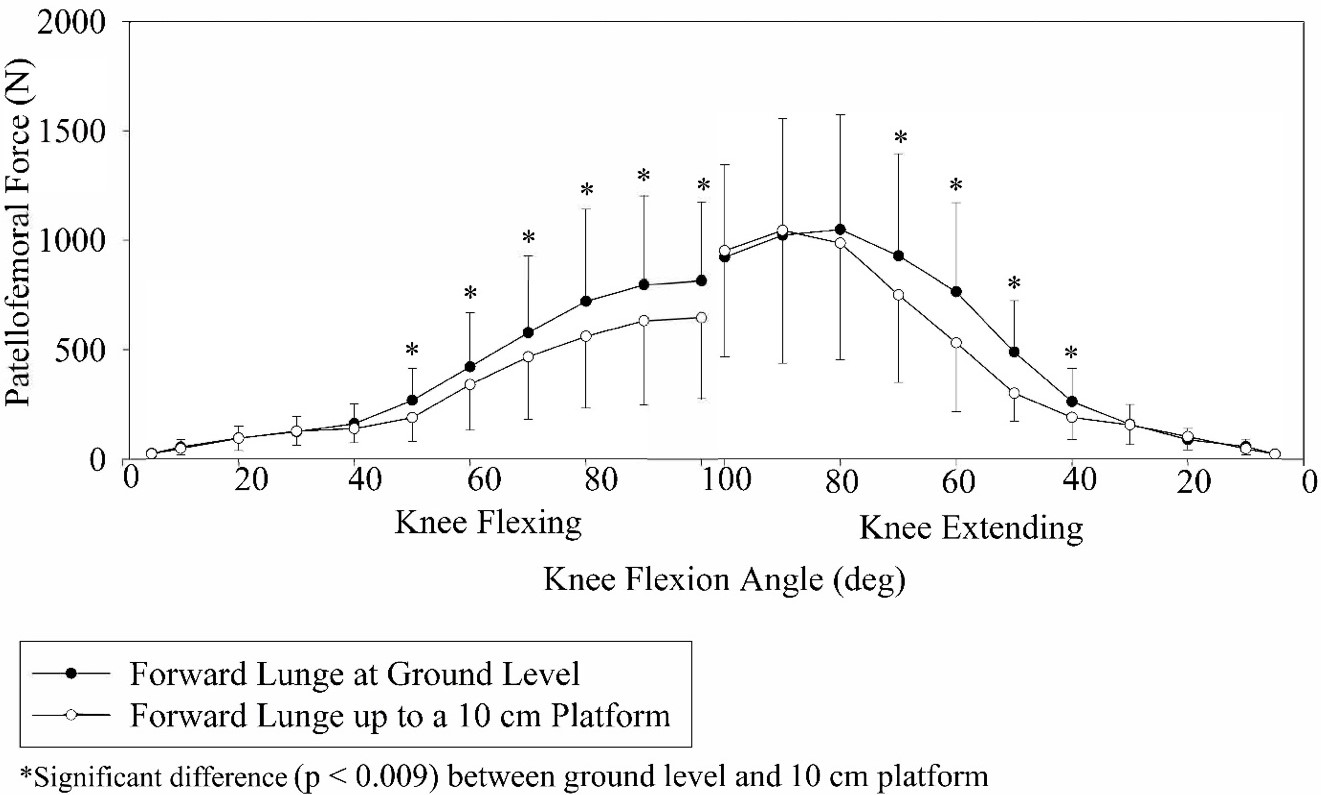
Comparing step height variations in the bodyweight forward lunge, patellofemoral loads were greater lunging at ground level compared to lunging up to a 10-cm platform between 40°–100° knee angles (Figure 5).16 A similar pattern was also observed while performing the side lunge at ground level versus up to a 10-cm platform.15 These data show a progression in patellofemoral rehabilitation, suggesting that lunging up to a 10-cm platform should precede lunging at ground level when the goal is to minimize patellofemoral joint loading.
_patellofemoral_compressive_force_in_lead_knee_for_forward_lunge_at_ground_level_.jpeg)
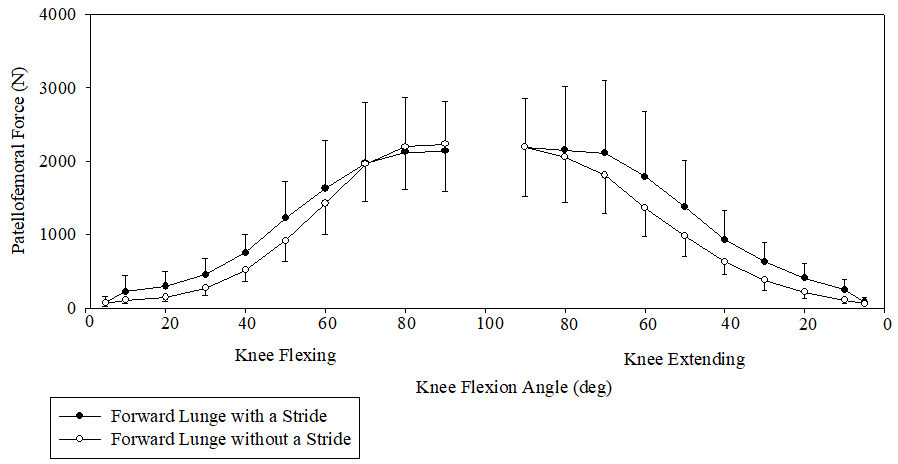
When comparing patellofemoral force and stress with a stride to without a stride during the forward lunge, between 10°-50° knee angles of the knee flexing phase and between 50°-20° knee angles of the knee extending phase patellofemoral force and stress were significantly greater with a stride than without a stride (Figure 6),23 and a similar pattern was also observed during the side lunge exercise.23 These data show a progression in patellofemoral rehabilitation, suggesting that stationary lunging (without a stride) should precede lunging by stepping forwards/sideways and pushing back (with a stride) when the goal is to minimize patellofemoral joint loading.
_patellofemoral_compressive_force_in_lead_knee_between_forward_lunge_with_a_strid.png)
There are several conclusions from examining the forward lunge data from Figures 3-6 when the goal is to initially minimize patellofemoral joint force and stress and then gradually progress loading: 1) initially employ a more functional knee flexion range between 0-50º; 2) then, progress to higher knee angles (0°–100°); (3) then employ a long step and higher knee angles (0°–100°) up to a 10-cm platform; and (4) finally, employ a long step and higher knee angles (0°–100°) at ground level.
Technique variations within squatting techniques can also affect patellofemoral loading. Patellofemoral force and stress were significantly greater at 90º knee angle in the 12-RM wall squat with the feet a short distance from the wall (causing the knees to translate anteriorly beyond the toes - referred to as wall squat short), with a peak force of approx. 3650 N, compared to the 12-RM wall squat with feet farther away from the wall (allowing the knees to stay over the feet - referred to as wall squat long), with a peak force of approx. 2900 N.24 During the 12-RM barbell squat, peak patellofemoral force and stress were greater with a wide stance squat (4313-4674 N at 80-90º knee angles) compared to a narrow stance squat (3958-4246 N at 80-90º knee angles), and mean patellofemoral force and stress was 15% greater in the wide stance squat than the narrow stance squat between 21-79º knee angles.2
Technique variations during the leg press can also affect patellofemoral loading. During the 12-RM leg press, peak patellofemoral force and stress were greater with a narrow stance leg press (4316-4809 N at 80-90º knee angles) compared to a wide stance leg press (3761-4389 N at 80-90º knee angles), and mean patellofemoral force and stress was 18% greater in the narrow stance leg press than the wide stance leg press between 19-91º knee angles.2
Concept #3: Knee Loading Varies Between Different WBE
Cruciate Ligament Rehabilitation
For PCL loading between different WBE, peak force was highest in the two-leg 12-RM barbell squat (1868-2212 N at 63-77 º knee angles), followed by the 12-RM leg press (1690-1726 N at 88-95 º knee angles), 12-RM wall squat (757-786 N at 80-90º knee angles), 12-RM forward and side lunges (641-765 N at 80-90º knee angles), 12-RM one-leg squat (414 N at 90º knee angle), bodyweight forward and side lunges (279-328 N at 70-80º knee angles), and level ground walking (160 N at 15-20º knee angles).1–8,11–14
PCL loading was greater in the 12-RM wall squat (259-757 N) compared to the 12-RM one leg squat (64-414 N) between 0-90º knee angles, while in contrast ACL loading was greater in the 12-RM one leg squat (22-59 N) than the 12-RM wall squat (0 N) between 0-40º knee angles.6 PCL loading was greater in the 12-RM barbell squat than the 12-RM leg press between 27-79º.2
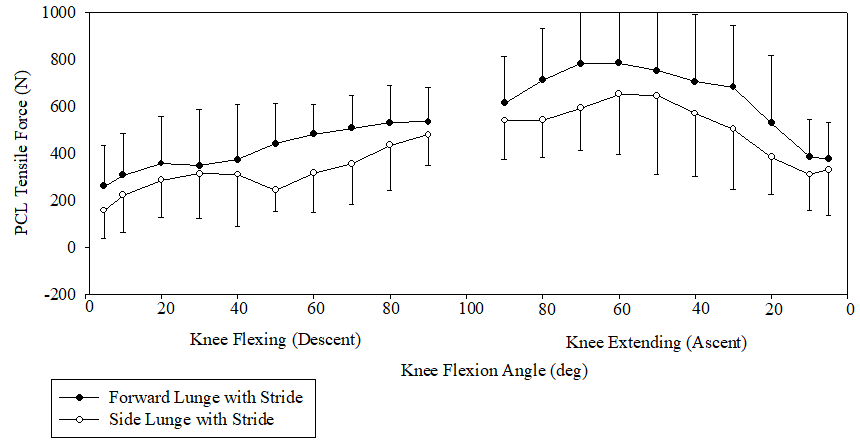
Cruciate ligament differences were also observed between the forward lunge and side lunge exercises performed both with bodyweight and with a 12-RM external load.8 PCL loading was greater in the 12 RM forward lunge than the 12-RM side lunge between 40-80º knee angles (Figure 7).8
_pcl_tensile_force_during_forward_and_side_lunges_with_a_stride_(step_forward_and.png)
Patellofemoral Rehabilitation
Differences in patellofemoral joint loading also occurred between the bodyweight forward and side lunge exercises when performed with step height variations, such as performing the forward and side lunge exercises at ground level versus performing the forward and side lunge exercises up to a 10-cm high platform (Figure 8).15,16
__side_lunge_at_ground_level_(b)__forward_lunge_up_to_a_1.png)
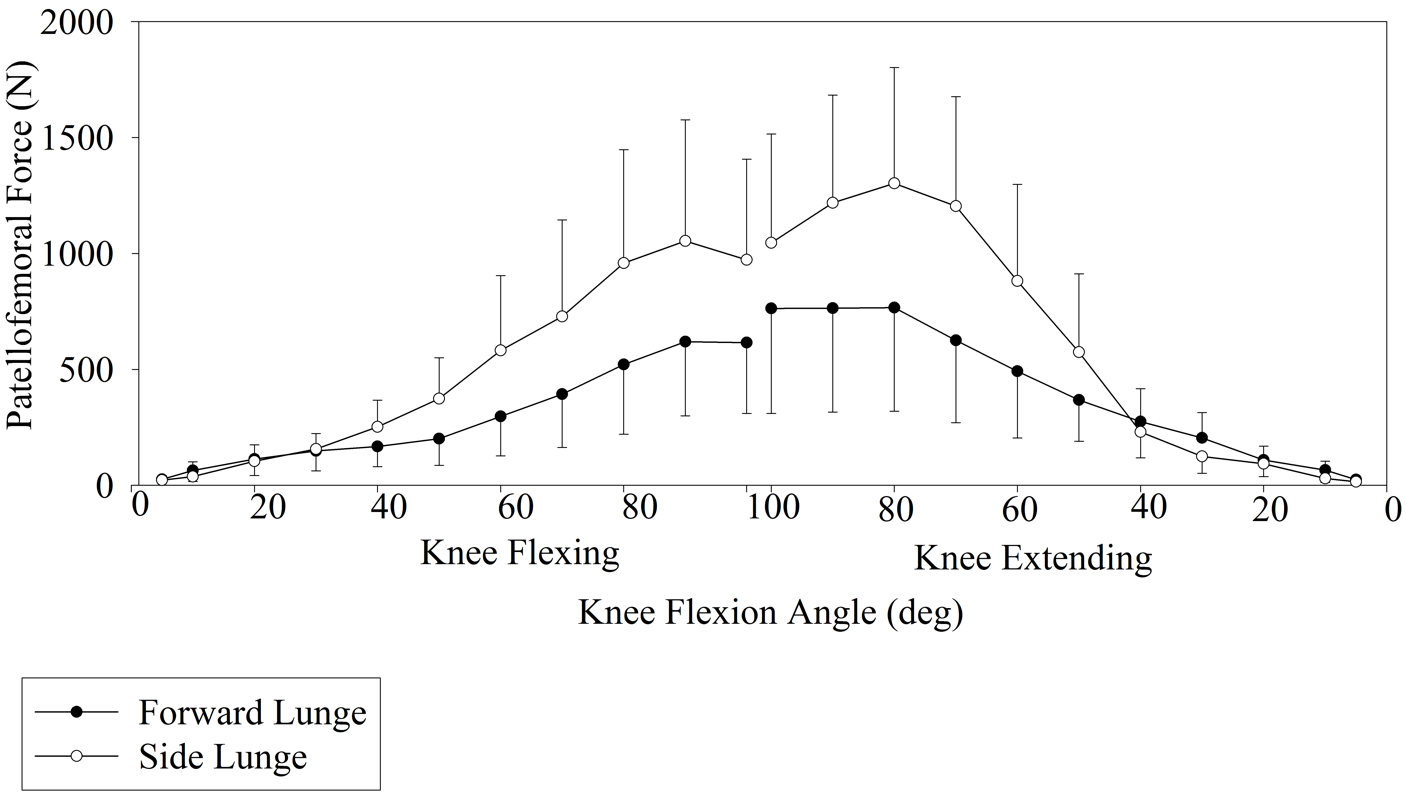
As shown in Figure 9 for the bodyweight forward and side lunge, at 10° knee angle during the lunge descent and at 10° and 30° knee angles during the lunge ascent, patellofemoral force and stress were significantly greater in the forward lunge compared to the side lunge.15 In contrast, at 40°, 50°, 60°, 70°, 80°, 90°, and 100° knee angles during the lunge descent and at 50°, 60°, 70°, 80°, and 90° knee angles during the lunge ascent patellofemoral joint force and stress were significantly greater in the side lunge compared to the forward lunge.15
_patellofemoral_compressive_force_in_lead_knee_between_forward_lunge_and_side_lun.png)
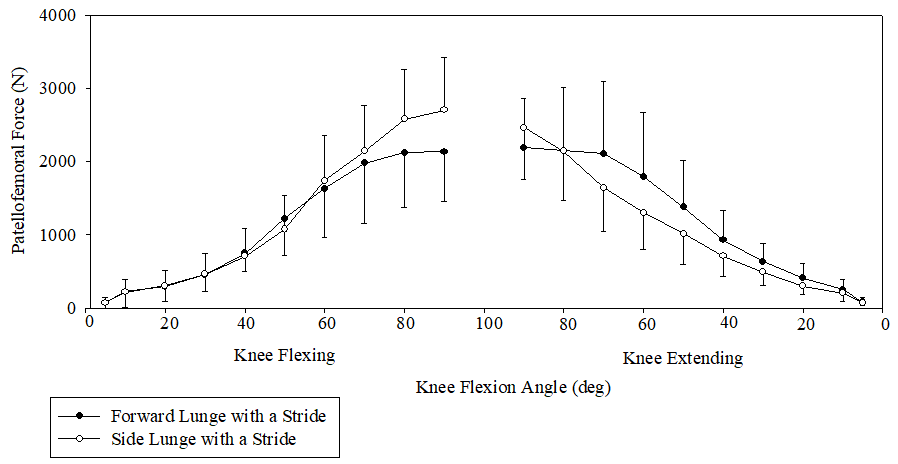
In contrast to the bodyweight forward and side lunge, during the 12-RM forward and side lunge the only significant differences found were between 80°-90° knee angles during the lunge descent and at 90° knee angle during the lunge ascent, in which patellofemoral force and stress were greater in the side lunge compared to the forward lunge (Figure 10).23
_patellofemoral_compressive_force_in_lead_knee_between_forward_and_side_lunges_w.png)
Patellofemoral force and stress were greater while performing the bodyweight side lunge (252-1302 N) compared to the bodyweight forward lunge (167-766 N) between 40-100° knee angles.15 When external resistance was applied, patellofemoral compressive force and stress magnitudes were greater during the 12-RM side lunge (2493-2668 N) compared to the 12-RM forward lunge (2161-2191 N) between 80-90º knee angles.
Peak forces for the 12-RM squat and 12-RM leg press were between 4500-5000 N at 90º knee angle, and not significantly different between each other.2 Patellofemoral force and stress were greater in the 12-RM wall squat (approx. 2100-3650 N) than the 12-RM one leg squat (approx. 1800-2800 N) between 60-90º knee angles.24
Concept #4: Knee Loading Varies as a Function of Knee Angle
Cruciate Ligament Rehabilitation
If we arbitrarily use a 0-100º knee angle range (0º = full knee extension), which is a common knee angle range of motion for most lower extremity WBE and NWBE, this range can roughly be divided in half for anterior cruciate ligament (ACL) loading (0-50º knee angles) and posterior cruciate ligament (PCL) loading (50-100º knee angles). However, for many WBE and NWBE, PCL loading can occur throughout the entire 0-100º knee angle range of motion. Peak PCL loading was generally greater at the higher knee angles (50-100º) than lower knee angles (0-50º), with peak PCL loading typically occurring at knee angles around 70-90º.2,4–8,11 In contrast, peak ACL strain/tensile force typically occurs at lower knee angles between 10-30º for both WBE and NWBE.2,6,10 For example, ACL strains during the isometric seated leg extension using a 30 Nm torque as resistance were 4.4% at 15º knee angle, 2% at 30º knee angle, and no ACL strain at 60º and 90º knee angles.10 Moreover, when tested at 30º, 50º, and 70º knee angles, squatting, lunging and step-up and step-down exercises had the greatest ACL strain at 30º knee angle.10 Moreover, it should be emphasized that peak ACL loading from both NWBE and WBE are of relatively small magnitudes, typically less than 150 N or 3.7% ACL strain (which is roughly the same as a 150 N Lachman test) for WBE, but higher (150-350 N) for NWBE,1–8,10,25,26 Therefore, if the rehabilitation goal is to minimize ACL or PCL loading, such as during the early phases after ACL or PCL reconstruction surgery, training with both NWBE and WBE would be appropriate starting with lower knee angles (e.g. 0-50º) for PCL rehabilitation and higher knee angles (e.g. 50-100º) for ACL rehabilitation.
Patellofemoral Rehabilitation
In general, for both WBE and NWBE, patellofemoral force and stress increase as knee angle increases and decrease as knee angle decreases. Therefore, when the goal is to minimize patellofemoral force and stress, performing exercise at lower knee angles (eg, 0-50º) is desirable, and progression to higher knee angles (eg, 50-100º) as more patellofemoral force and stress can be tolerated later in the rehabilitation process.
Concept #5: Knee Loading Increases with Increased Knee Anterior Translation Beyond Toes
Cruciate Ligament Rehabilitation
For ACL rehabilitation, anterior knee movement of 8-10 cm or more beyond the toes may increase ACL loading during squatting, lunging, leg press, and other WBE.4,6–8 Moreover, squatting with the heels off the ground, which typically results in increased anterior knee movement beyond the toes, resulted in over three times ACL loading compared with squatting with the heels on the ground.4,11
ACL loading was significantly greater in the one-leg squat, in which the knees moved forward beyond the toes 10±2 cm, compared to performing the wall squat long with the knees positioned over the feet.6 ACL loading was significantly greater in the 12-RM forward lunge short (using a short step, in which the knees moved forward beyond the toes 9±2 cm), compared to the 12-RM forward lunge long (using a long step, in which the knees stay over the feet throughout the movement).4,5,7 Moreover, squatting with a more erect trunk position compared with squatting with a 30-40º forward trunk tilt position tends to cause more anterior translation of the knees beyond the toes, as well as greater quadricep activation (which increases ACL tensile force at lower knee angles) and less hamstring activation (which results in less unloading of the ACL).2,6
Patellofemoral Rehabilitation
Patellofemoral force and stress were significantly greater at 90º knee angle in the wall squat short (knees translate anteriorly beyond the toes), with a peak force of ~3650 N, compared to the wall squat long (knees stay over the feet), with a peak force of ~2900 N.24 At the lowest position of the wall squat short (90º knee angle), the knees translated beyond the toes 9±2 cm, compared to the knees being above the ankles and over the feet for the wall squat long.24
Conclusions
It has been demonstrated that both cruciate ligament loading and patellofemoral loading varies between WBE and NWBE, varies with technique variations within WBE and NWBE, varies between different WBE, and varies as a function of knee angle. Understanding how varying techniques within and between WBE and NWBE affect cruciate ligament and patellofemoral loading may help clinicians better prescribe WBE and NWBE in a safe and effective manner during cruciate ligament and patellofemoral rehabilitation.
Disclosures
The author of this manuscript affirm we have no financial affiliation (including research funding) or involvement with any commercial organization that has a direct financial interest in any matter included in this manuscript. The authors of this manuscript also affirm they have no conflict of interest of any kind.