




INTRODUCTION
The sliding sports of Bobsled, Luge, and Skeleton require an athlete to tactically navigate a steeply pitched, winding, icy track surface while reaching speeds over 93 mph.1 Sliding athletes must develop fine motor skills which allow them to navigate a track under variable circumstances which may include, at times, subzero temperatures where the slightest error may result in catastrophic injury. In addition, they must also adapt to withstand persistent exposure to varying levels of gravitational forces from taking more than fifty runs during some training weeks across a season that is often six months long. Each sport type is variable and nuanced, from equipment utilized to technical requirements,1 which will be detailed in various sections of this commentary. The existing variance between each sliding sport needs to be considered to gain an understanding of the sport demands and unique variables influencing health and performance across each discipline, all of which will be discussed. Given the technical variability between sliding disciplines, understanding common injury patterns and sport demands within disciplines is beneficial when developing medical management plans. However, research-supported recommendations and literature focus on the sliding sport athlete are lacking. As a result, recommendations to the field in developing a multi-faceted medical management program for this athlete population are mostly anecdotal and rely upon field experience. Therefore, the purpose of this commentary is to describe the unique challenges associated with the medical management of sliding sport athletes and offer recommendations for developing an integrated approach for mitigating injury risk and optimizing performance within this population.
TECHNICAL ANALYSIS
The sports of Bobsled, Luge and Skeleton vary across many technical aspects. From variations in sled architecture and start/sliding techniques to training programs and race categories, the unique sports demands are described to provide the reader with an understanding of each sliding sport. Additionally, special consideration is given towards the start as a competitive start is widely considered to significantly increase the chances of overall success in sliding sports.2–4 While biomechanical patterns in the start may vary between each sliding sport, with the lower body extremities more involved in a bobsled and skeleton start compared to the upper body in luge, the common objective is to accelerate the sled with precision and speed to optimize post-loading velocity.5
Bobsled
Bobsled is composed of three disciplines with sleds varying from approximately 2.80 meters in length (mono bob) to 3.80m in length (4-man bob). Some athletes participate in more than one discipline.6 Each discipline must abide by maximal weight restrictions for competition. With crew, the cumulative weight of the women’s monobob must be less than 248kg, 2-Man bob 330kg (women’s) and 390kg (men’s), and 4-Man bob 630kgs.6 Positions in the sled include the driver, who engages steering below the cowling (protective covering) in the front of the sled to navigate the track, followed by push athletes who sustain a head tucked and maximally trunk flexed sitting position in the sled once loaded. The push athlete in the rear of the sled is considered the brakeman/woman and is responsible for braking inertia of the sled on the runway once crossing the finish line. Athletes push their bobsled over approximately 50 meters while on a grooved surface before transitioning into the sliding phase.6
Start Technique
The Bobsled start is composed of the introductory phase, the pushing/reversing phase, the acceleration/thrust phase and the achievement of maximum speed.7 In monobob, the pilot pushes from the rear of the sled while grasping two handles formed into the cowling of the sled with the elbows, trunk and lower quarter in a semi-flexed position while their feet are grounded on a board attached to the track.8 This same technique is applied by the breakmen/women in 2-man/woman bobsled, however the position of the pilot and other push athletes in 2-man/woman and 4-man bobsled vary as these athletes are positioned to the side of the sled in a staggered stance behind a lateral push bar.
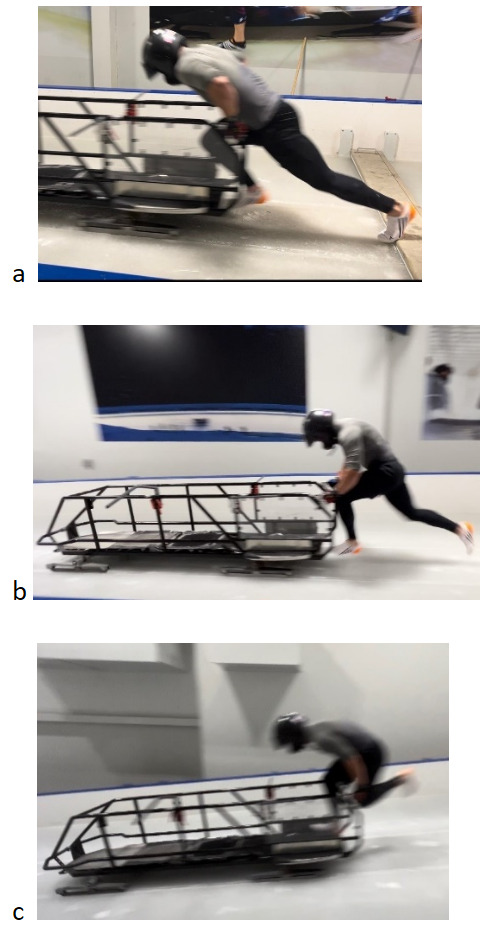
The introductory, or “hit” phase (Figure 1a), typically occurs with explosive trunk and hip flexion followed by rapid lower limb extension as the athlete pushes off the start block. While pushing, athletes focus on maintaining forward propulsion as they push the sled without shedding speed (slowing) from exerting too much downward or inward force on the push bar.8 This transition into the pushing phase incorporates the first driving step occurring simultaneously with the initial propulsion of the sled to break inertia. As the sled is pushed from the block, athletes maintain partial trunk flexion while driving one foot forward in a shortened stride that lengthens as they overcome the initial inertia, increase distance from the block, and enter the acceleration/thrust phase (Figure 1b).8 The athletes achieve maximal speed as the sled passes beyond the “crest”, or the point of increased slope. Beyond the crest, the sled hits a critical intersection where gravitational forces and the speed already produced overcomes athletes’ capacity to add substantial increases in momentum to the sled, at which point the pilot, followed by brakemen/women, load (Figure 1c) into the sled in a choreographed manner, from front to back, that minimally affects speed.8 Due to the combination of overspeed, which results from the combination of maximal speed being achieved in combination with gravitational influence as the sled transitions down the crest, and an increased trunk extension moment while pushing as athletes prepare to transition into loading the sled, the biomechanical demand on the hamstring and posterior chain muscles is increased which can be a catalyst for acute muscular injuries.
_hit_phase__b)_acceleration_thrust_phase__c)_load_phase.png)
Equipment
Bobsled athletes wear a full-body synthetic race suit under which is a required Kevlar burn vest to mitigate the severity of ice burns in the case of a crash, helmets meeting specific safety standards, and low-cut ice sprinting spikes (Figure 2) composed of a minimum of 250 micro-spikes located on the forefoot plate to provide traction.6 Face shields and goggles are typically worn exclusively by the pilots of the team.

Luge
Luge is comprised of four disciplines: singles and doubles for both men and women as well as the mixed event and team relay.9 Sled weight is also regulated with a single sled minimum-maximum weight of 21-25kg and 25-30kg for doubles sleds.9 These weights may vary slightly at the youth and junior class levels.9 Luge athletes slide down the track on their backs with their chin in a slightly tucked position and feet against the kufens, or steels, that curve upwards in front of the sled, where slight pressure is applied for steering while maintaining stability in their lower legs and shoulders within the sled shell. At the finish, the sled is decelerated by the athlete transitioning to an upright sitting position with their booties in contact with the ice surface while lifting the front of the sled.
Start Technique
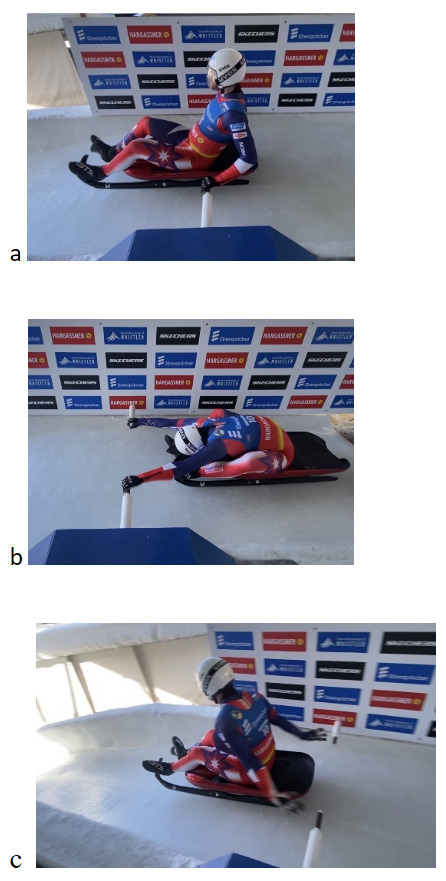
The six phases of the Luge start are the block, the compression, the pull, extension, push-off then paddles. This is where each Luge athlete uses their explosive power to gain the most traction and build speed to descend the track. The block phase (Figure 3a) begins with the athlete rocking the sled forward past the start handles while leaning the trunk backwards. Next, is the compression phase (Figure 3b) where the athlete ballistically pushes backwards on the handles, entering full hip flexion and shoulder flexion. This allows the athlete to utilize the stretch-shortening cycle to move into the pull phase. During the pull phase, the athlete tenses and locks in upper body musculature, engages the hips and pulls against the start handles which then transitions them into the extension phase, which is the longest phase of the start. The extension phase (Figure 3c) occurs when the athlete begins forward propulsion with the hips and extends the trunk upright to a 90-degree angle and ends when the hips are in line with the start handles. Immediately following is the push-off phase (Figure 3c), which is continued forward propulsion by pushing off the start handles.
_block_phase__b)_compression_phase__c)_extension_into_push-off_phase.png)
The athlete then finishes the start sequence with the paddle phase which typically consists of three to six paddles using the hands on the ice, depending on the track length (Figure 4).

Once the athlete has finished their specific number of paddles, the athlete(s) settle into their sliding position on the sled and complete their run.4 For the start in a doubles sled, the bottom athlete, or one positioned closer to the back of the sled, grabs and pulls on straps instead of handles. The straps are attached to the top athlete’s or driver’s suit behind the arms to connect both athletes as they work together to propel the sled forward from the start position.
Equipment
Luge athletes wear a full body synthetic race suit, a UVEX helmet with face shield, race booties and specialized 4mm race spikes (Figure 5) on their pointer, middle and ring fingers to gain traction during the paddle phase of their start.9

Some athletes also wear weight vests or shorts to meet their allotted weight maximum, of which was referenced previously. The sleds for Luge differ between singles and doubles disciplines as they are tailored to the athlete who is in contact with the sled. A singles athlete is the only body on the sled, therefore that athlete is measured, and the pod (sled frame) is made to fit their body type and height, whereas for a doubles sled, the bottom athlete is the one who is measured, as this athlete is in contact with the sled.
Skeleton
Skeleton consists of a single slider and no combination disciplines. The maximum combined weight for both the sled and athlete is 120kgs for men and 102kgs for women with the maximal sled weight alone set at 45kgs for men and 38kgs for women.10,11 Similar to Bobsled, the athlete pushes their sled from a sprinting start for 50 meters before loading and transitioning into their sliding position which consists of lying stomach down on the sled with the chin just a few inches off the ice and head in a neutral position while steering with subtle pressure applied from the upper torso into the sled frame.
Start Technique
The Skeleton start can be divided into five distinct phases: block, drive, transition, maximal pushing velocity, and load. Specific to Skeleton, notable physical and technical parallels have been drawn between the initial acceleration in sprinting and pushing.12 Additionally, sprint velocity, which is determined by step frequency and stride length, is an aspect that coaches aim to enhance through training to optimize post-loading velocity.13 The block phase commences with the athlete gripping the saddle, or sled frame, with one hand to stabilize the sled flat down on the ice while positioning their feet in a split stance, with the back foot on the starting block and the front foot resting on the ice, resembling a sprint block setup. Subsequently, the athlete loads the hip through flexion and extension, rocking the sled forward and backward to break its inertia, a process that may be repeated several times to prepare for the next phase. The drive phase (Figure 6a) commences with hip extension, propelling forward as they push against the block, utilizing their center of mass to accelerate the sled. The angles of the torso and shins during this phase exhibit similarities to those observed in sprint acceleration as the athlete retracts the foot for the initial steps.12 This phase concludes when the shin reaches a vertical position during swing phase relative to the ice. In the transition phase, there is a gradual increase in both step frequency and stride length. Athletes may adjust their step count based on the track’s profile,14 potentially due to insufficient strength-speed qualities to maintain sled acceleration over the gradient. During the maximal pushing velocity phase (Figure 6b), both step frequency and stride length peak prior to loading, with the athlete positioned at the highest gradient of the track profile. The load phase (Figure 6c) represents the final opportunity for the athlete to generate velocity, as they bring their hands across the saddle in front of their torso, establishing a stable position to propel forward with the outside leg onto the sled.
_drive_phase__b)_maximum_pushing_velocity_phase__c)_loading_phase.png)
Subsequently, the athlete adopts a prone position (Figure 7) on the sled, gripping the lower part of the saddle. Typically, the start is completed within 14-18 steps depending on the track profile.

Equipment
Skeleton athletes wear a full-body synthetic fabric race suit and, like bobsled, specialized low cut ice sprinting spikes (Figure 2) with a minimum of 250 spikes in the forefoot to allow the greatest amount of traction on ice.11 Skeleton helmets are full coverage with a uniquely shaped design to allow for both chin protection and cervical extension which support the sliding position and in meeting established certification standards.11 Skeleton athletes are not required to wear burn vests.
SLIDING TRACK CONSIDERATIONS
There are currently 15 tracks on the luge competitive race circuit, and 14 on the bobsled-skeleton competitive circuit.15,16 Track length, top speeds, gravitational force influence, maximum gradient, average gradient, and curve exposures vary from track to track, influencing the variability of technical and physical demands that exist from track to track (Figure 8).
The initial characteristics of each track are distinct and vary in profile, which influences individual starting strategies. Traditionally, Bobsled and Skeleton start on a 2% gradient, accelerating the sled to the 15m first official timing eye, gradually increasing speed down the 8-12% gradient track before loading into the sled.6,11 A split time is recorded at 65m at the second official timing eye. In contrast, luge start ramps feature a steeper gradient of 20% to 25% and range in length from a minimum of 10m to a maximum of 30m, this may vary depending on upper or lower start in the track. The first official timing eye must be installed no further than 5m after the start handles and the second sequentially 100m to 150m further in the track.9 These track characteristics play an influential role in athlete skill development strategies and return to sport from injury planning.
SLIDING ATHLETE HEALTH MANAGEMENT
Injury and Illness Epidemiology
Given the combination of speed and navigation on a curved, icy track, sled crashes across all three sliding sports are a realistic probability. The average rate and severity of injury may change with each sliding track due to differences in top speeds, G-forces, and overall track technicality. Reviews of global occurrence studies at the Winter Olympics from 2014 through 2022 show acute injury occurrence/recurrent injury rates varying from 5-11% for Luge, 8-18% for Skeleton, and 14-18% for Bobsled.17–19 The 2016 Youth Olympic Winter Games in Lillehammer in 2016 resulted in overall injury rates of 14% for Bobsled, 3% for Skeleton, and 35% for Luge.20 Discrepancies between youth and Olympic level athlete injury rates may be due to competitor field size, experience level, and track technicalities. A retrospective study encompassing 43200 runs over four years for the Whistler Sliding Center showed that the overall injury rate was 0.5%.21 Of the injuries found 20% were concussions, 39% abrasions, 14% fractures, 20% strains, sprains, and 5% miscellaneous.21
From a musculoskeletal injury perspective, overuse conditions with gradual onset and thigh tendon rupture were identified injury conditions, in addition to head injuries and concussion in the sport of Bobsled.17,22 Additionally, the rate of injury occurrence was higher in training than competition.17 Furthermore, Bobsled was identified as having a higher injury risk whereas Luge had statistically lower injury risk when compared to other Winter Olympic sports.17,22
The incidence of head injury and concussion within sliding sports has not been completely described despite reported incidences.1,22 There appears to be a growing awareness and recognition of symptoms, typically in the form of headaches and fogginess, which may occur in response to exposure to bumpy tracks and/or multiple runs.23 Although head injuries and concussions occur in sliding sports, further research is required to determine the exact incidence and prevalence of these injuries as well as underlying causes for symptoms that manifest.
Additional consideration regarding environmental conditions, in particular cold weather, must be given within these athlete groups. Given the focus on optimizing aerodynamics within competition, athletes only wear helmets, speed suits and thin gloves as protection against the elements while sliding at over 80mph in sub-freezing temperatures. Therefore, hypothermia is a realistic possibility and must be considered within management strategies that are implemented.
Specific Injury/Illness Management Considerations
Illness is another contributing factor of which providers must effectively manage to ensure that contagion, when present, does not spread to other members of the team and hinder performance. Reviews of global occurrence studies at the Winter Olympics from 2014 to 2022 indicate illness rates varied from 3-11% for Luge, 8-28% for Skeleton, and 5-14% for Bobsled.17 Female sliders consistently showed a higher occurrence of illness compared to males. Across the sliding disciplines, Skeleton and Bobsled had a high rate of illness, in particular affecting the respiratory system, compared to other winter sports whereas Luge had the lowest rate of illness.17,22
Both unique injuries and medical considerations exist within sliding sports. Medical providers must develop a system for extracting and triaging athletes out of cold, icy tracks where up to four athletes may have severe injuries and be unable to move due to their injuries or being trapped by the sled. This requires providers to be both adequately informed of venue emergency procedure protocols and prepared with the appropriate attire befitting of responding to athlete injuries in a cold weather and sliding track environment, such as traction cleats or crampons and outdoor winter gear.
Team medical providers work closely alongside track personnel and emergency medical technicians to ensure safety of the athlete in the instance of a sled crash. Critical attention must be paid to movement and location of the sled within the track following a crash, regardless of location of the athlete, as a moving sled imposes significant harm upon responders and the athlete(s) involved. Once the sled’s momentum has ceased, typically in the lowest gravitational point of the track, it is then safe to enter the track under the direction of track personnel to respond to the involved athletes. Initial assessment should screen for alertness, orientation and life-threatening trauma prior to more detailed neurological and orthopedic screens. In a suspected case of cervical spine injury, it is critical that any obstruction, such as the sled or a responsive teammate on top of an unresponsive one, is removed with caution in order to allow for proper assessment and management of the injured athlete, including spine motion restriction via use of a cervical collar as well as either a scoop stretcher or spine board for hospital transport. Given the risk for hypothermia, thermal blankets should be available for transport. It should be noted that in any crash, in particular those occurring during Bobsled, there is a possibility of athletes ejecting and/or losing contact with their sled further up the track so multiple medical support teams located at various points along the course ensures more timely response in these situations. Streamlined communication and alignment within the response plan by all involved stakeholders is critical to the success of implementing emergency protocols for sliding sports.
“Ice burns” are friction burns that occur when sliders collide with the wall or are pinned against the ice from their sled during a crash for prolonged periods, which can be a more common occurrence when the heavier bobsleds crash. These can range from third to first degree burns with large surface areas being affected. While some athletes may be wearing burn vests, however, the vest does not protect the shoulders, arms, or legs, which are the most exposed body regions.
In the cases where an intervention greater than a bandage is needed, similar treatment methods for friction burns are used to treat ice burns which entails 48-72 hours of silver hydrogel dressing followed by one to six weeks of hydrogel dressing depending on the severity.24,25 First degree burns require immediately cooling the burn with cold running water for 10-15 minutes followed by cleansing with soap and water and placement of a cold compress used for keeping the burn area clean.24,25 Second degree burns require cooling the area with cold water and ensuring that it is cleaned with soap and water as well as applying an antibiotic ointment.24,25 Third degree burns require debriding and cleansing before the application of a silver sulfadiazine cream.24,25 Absorptive, antimicrobial dressings can be applied and secured with poly stretch bandages on both second and third degree burns to keep the area covered for 24-48 hours post injury.24,25
Return to Sliding Considerations
Standardized return-to-play protocols for a variety of medical conditions, including concussion26 and musculoskeletal injury, are challenged when sports-specific phases of these protocols are re-introduced, especially in-season. Bobsled and Skeleton athletes can re-introduce sprint drills and heavy sled pushes as an alternative for starts. Some training centers may also have ice-surface start houses which allow sleds for all three sliding sports to be used on ice in a controlled setting without going down a track. However, these training centers are niche and unlikely to be available while racing during the season which requires athletes, coaches, and medical providers to improvise. Ultimately, athletes must be exposed to sliding down the track. In theory, it may seem more appropriate, from a return to sport progression standpoint, to transition athletes from lower start points on the track compared to immediately returning to sliding from the top. However, the athlete would then have to alter their steering from their typical or normal to compensate for entering turns at a lower speed which potentially may ultimately increase crashing risk. Additionally, logistical complications such as track availability during race training periods, the track being properly staffed by track crews and medical personnel, limited track runs per training session and, in the case of Bobsled and Luge, the availability of additional athletes to fill a sled for training runs influences the process of building sliding tolerance in an abbreviated window of time prior to the next race competition. This poses a unique challenge for the sliding athlete that may not be encountered by other sports.
For return to sliding sport following injury, progression and timing depend on the injury type and sliding discipline demands. For example, a Luge athlete may likely have an earlier return to sport date compared to Bobsled and Skeleton athletes following a hamstring injury due to the technical demands of each sport discussed previously. Due to the sprinting requirements and lower extremity demands in the sports of Bobsled and Skeleton, considerably greater stress is placed on the posterior thigh musculature compared to Luge and as a result a longer rehab course would be required to gradually build adaptive soft tissue loading capabilities before returning to sport (Appendix A). Alternatively, in the case of a shoulder strain or instability, a Luge athlete may require more extensive shoulder rehabilitation to regain the necessary range of motion and strength required within the sport (Appendix B). Consideration towards phases of the start, sled transition, sliding position and dynamic loading capacity of the injured soft tissue must be considered when building out progressions in both rehab and return to sport specific training.
Following concussion, athletes should be guided through a six-step return to sport progression according to the guidelines set forth by Patricios et al.26 These progressions would include gradual exposure to light and medium intensity exercise to assess response before transitioning into sports-specific non-contact activities prior to higher intensity, contact activities based on sport demands.26 For the sliding sports, additional consideration must be given towards the exposure to gravitational and acceleration forces within the sport. While the best preparatory exposure to these demands within sliding is sliding itself, the athlete can be exposed to a variety of plyometric, body roll and proprioceptive exercises designed to assess an athlete’s ability to tolerate multidirectional rotational and gravitational forces on land before transitioning back into sliding (Appendix C).
TECHNICAL DEVELOPMENT AND PERFORMANCE OPTIMIZATION
Strength Programming
It is essential for strength and conditioning professionals to establish a technical framework aimed at developing biomechanical qualities that enhance start performance. This can be accomplished through clearly defined objectives that align strategically with the training program’s goals.27 However, with evidence-based guidance for sliding sport strength programming being limited, practitioners must be attentive to individualizing program recommendations based upon the needs of the athlete(s), with specific consideration towards the technical demands within each sport.28,29
Variability in training exists between sliding sports, with Luge emphasizing upper body physical development, in contrast to Bobsled and Skeleton. Colyer et al. identified three critical biomechanical qualities that predict start potential in Skeleton athletes: sprint ability, lower body explosive strength, and strength-power characteristics.5,30,31 Similar correlations have been noted in Bobsled, including sprinting, anaerobic power, and isokinetic knee strength to start capacity.28,29 It is recommended that Bobsled and Skeleton athletes incorporate resistance training to build strength and power in addition to speed training methods like sprints and plyometrics to improve explosive power in the lower body.32 As Luge athletes improve their technical efficiency, the significance of upper body strength in start performance increases.4 Additionally, research indicates that isometric bench pull strength is a key factor affecting maximum push-off speed in various tests assessing physiological elements of the start.3
Furthermore, given the characteristics of gravity-affected sports, integrating hypertrophy training could lead to improved finish times, as evidence suggests that the mass of the athlete-equipment system impacts winning times in Skeleton and Luge.33 Skeleton athletes can experience sustained G-forces of up to five Gs during a corner and significant vibrations due to bumps in the ice.34 Similar longitudinal and centrifugal forces will also impact Bobsled and Luge athletes.35 Due to the required head position throughout a run, it could be beneficial to incorporate neck stability/strengthening programs to enhance neck girth and cervical stabilization which may help reduce head accelerations and thereby lower the risk of concussion.36
Practitioners should exercise caution when considering the implementation of strength and conditioning programs as improper training can negatively impact start performance if training volume is not managed appropriately. Athletes typically undergo several months of off-season training, starting with higher volume, lower intensity, and lower specificity, and then transitioning to lower volume, higher intensity, and higher specificity as they approach the in-season competition phase. It is important for athletes to continue training strength, power, and speed qualities throughout the season to maintain a competitive start. Additionally, periodic medical assessments and fitness profiling, including analysis of strength, force production, and biomechanical loading patterns is helpful in both screening for patterns indicative of higher injury risk as well as developing programming individualized to each athlete.
Visualization and Mental Imagery Training
Success in sliding sports relies heavily on the athlete’s mental representation of the tracks on which they race. They must build and maintain a memory for each curve, the challenges therein, and their tactical approach related to how navigation of one curve sets them up for the next. Given track runs per session and actual sliding time can be limited during competition weeks in-season, athletes have limited time to learn and relearn each track on tour and build robust mental models. To boost learning, memory, and performance, sliding sport athletes rely on a combination of film, track walks, and motor imagery, or, to use sliding sport terminology, “mind runs.”
Mind runs are a standard feature of sliding sport training. Athletes close their eyes and visualize sliding down the entire track or sections of it, seeing and feeling themselves navigate each curve and often moving their upper bodies to “steer” subtly – imagining their optimal line. Athletes perform mind runs in between actual training runs, before races, in conjunction with watching film, or any time they wish to mentally rehearse. Some coaches encourage athletes to do mind runs while in a sled to create a higher fidelity sliding experience. Athletes may do abbreviated mind runs shortly before approaching the start line to refresh performance cues for a track’s most consequential curves. A large body of research suggests that motor imagery improves motor representations, or organized mental blueprints for everything the motor task requires, of complex motor tasks37 and motor performance38,39 while also improving sport-related confidence.40
When conceptualizing mind runs, the Physical, Environment, Task, Timing, Learning, Emotion, Perspective (PETTLEP) model of imagery41 and similar research38,40 should be considered. Incorporating multiple senses, vividly setting the scene of the track while including other people and surroundings from a first-person perspective, incorporating physical cues and movements through dynamic motor imagery, striving for at least a portion of mental reps to occur at “racing speed”, and calibrating imagery duration and complexity to the athlete’s current level training or performance are all strategies that can be implemented to optimize the effectiveness of the mind run. For example, if an athlete has just returned to pre-season sliding after months off the track, their imagery may simply focus on the feeling of relaxation they want to achieve in the sled. As the athlete completes more runs, they may use imagery to rehearse more complex approaches to specific curves and specific lines they want to draw on the track. This may also include the athlete wearing their helmet and speed suit, getting into sliding position on a sled and mimicking precise steering movements to navigate a specific curve or set of curves.
For athletes who are less experienced with complex and structured motor imagery, it is helpful to start small and build images gradually. Layered stimulus response training (LSRT)42 is an approach that systematically layers progressively complex stimuli to help athletes generate and control images.43 Further, research suggests that LSRT may lead to greater improvements in the performance of complex motor skills, like golf putting, relative to standard imagery practice.42,44
The basic steps of LSRT are image, reflect, and develop.44 A sliding sport athlete may start by focusing solely on short-duration, low-complexity scenarios, like the moments before their start and the start itself. The athlete will begin by building an image – setting the visual scene of a specific track, feeling their speed suit on their body and the cold temperature on their skin. They should hold onto this image until it becomes fuzzy or they lose control. Then, exit the image and reflect. How vivid was the experience? Did they experience any psychophysiological changes in conjunction with the imagery scenario (e.g., increased heart rate or sweating before the start of a race)? What senses (e.g., sound) or sensory details (e.g., spectators) were missing? The athlete then re-enters and further develops the original image - picking a small number of additional sensory cues and layering these on top of the imagery foundation they built. The athlete may repeat this process and gradually increase the duration and complexity of images as they gain greater imagery mastery.
INTEGRATED SUPPORT APPROACH
In elite and high-risk sports, fostering an integrated approach is critical to the success of not only the athletes who are being supported but also the collaborative efforts across various stakeholders, such as medical providers, sports psychologists, dietitians, strength coaches and technical/sport coaches, involved in the process of optimizing athlete health and availability. Effective communication strategies not only optimize the integration of knowledge and experience of involved stakeholders but also enhance athlete health.45 An ideal transdisciplinary model is one in which athlete injury updates and performance development goals are communicated across all disciplines involved while integrating athlete voice in the processes of rehabilitation and goal planning to collaboratively develop treatment and return to sport progression plans while also identifying opportunities for appropriate referral to additional providers. Various examples of incorporating a transdisciplinary framework within sliding athlete care might include developing a psychologically-informed rehabilitation protocol for an athlete who is anxious about returning to sliding after a head injury, incorporating vestibular or visuomotor drills into strength and conditioning programming through collaboration between medical providers and coaches, and implementing the expertise of sport dietitians and psychologists to help an injured athlete optimize fueling for performance while coping with sport-related body weight and shape pressures. Environments which foster collaboration, trust, and clear communication among staff in these examples, while providing athletes with a positive vision and consistent support, are likely to yield better outcomes, such as reduced injury rates, improved adherence to training programs, and increased availability.45,46 Cohesion within the athlete support team will not only foster efficient communication practice but could also allow for both athletes and support personnel to best navigate challenges as they arise, such as injury or perceived competitive environment “failure”.46
SUMMARY
Sliding sport athletes are exposed to a technical and high-risk competitive environment. Given the nuance between each discipline, it is important for the medical provider to gain familiarity with sport demands and potential challenges which may be encountered when managing health and performance of the sliding sport athlete. These considerations include start and sliding techniques, equipment and variability among tracks on an international competition circuit.
An understanding of emergency procedures, injury and illness epidemiology, and return to sport considerations unique to both sliding sports and track venues is an important component of mitigating risk and optimizing healthcare of the sliding athlete. Strategically planning strength and conditioning programs while integrating mental imagery practice to best meet the needs of the sliding athlete can positively influence performance. A holistic, transdisciplinary approach should be integrated to best leverage the knowledge and expertise of medical providers, coaches and support staff in optimizing athlete health and performance.
Conflicts of Interest
The authors declare no conflict of interest.